I managed to get to speak to my daughter who was passed her mobile phone kept locked away in the office right now which according to LINCOLNSHIRE PARTNERSHIP TRUST IS IN LINE WITH HUMAN RIGHTS.
I was worried for her safety the other day having heard she was having an episode.
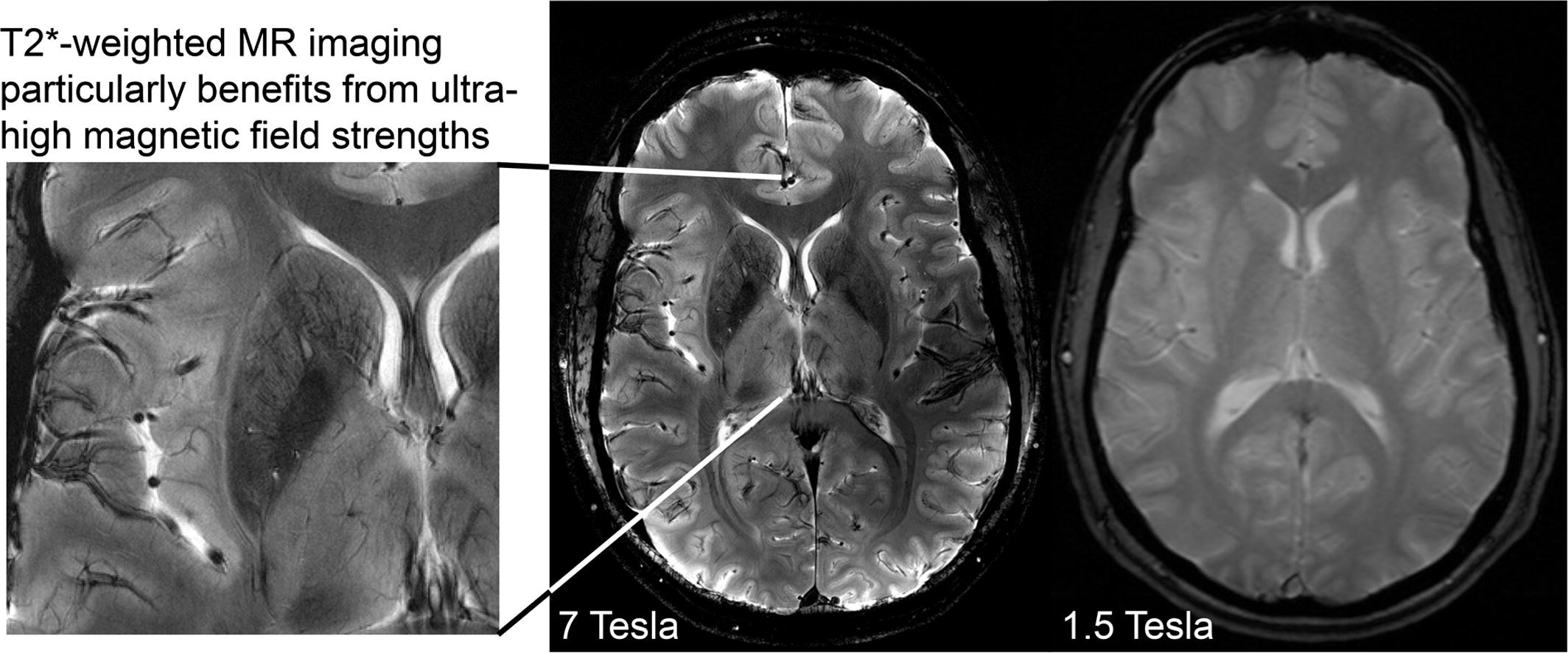
I am going to write all about the injury my daughter is suffering and the frequent episodes and constant rapid tranquilisations Castle Ward are giving on virtually a daily basis. I now want all the scans re-looked at as nothing can be relied upon under Lincolnshire who only have a 1.5 scanner. In my previous blogs I have included some interesting research papers on 1.5 MRI as opposed to Tesla 3. A Tesla 3 is why the private scans I had done revealed details not visible on a 1.5 scanner and I am warning everyone to check on which scanner their Trust has.
The restrictions are supposed to have ended on 5 February but continue with phone locked away and visits heavily restricted 2-1 supervised. Elizabeth said she misses not being able to listen to music on her phone. I am going to invoice LPFT for the contract as it is not being used. It was during my conversation with Elizabeth that she mentioned Castle Ward want to film her on the advice of the Neurologist when she has an episode. How can this be accurate and I want things accurate and to be 100% sure and the only way for this is for Elizabeth to be referred under S17 leave to Sheffield where they have a Tesla 3 scanner and a proper ward for neurology. This would need to be granted by Dr Waqqas khokhar as currently she has no leave entitlement whatsoever. Elizabeth said she did not want to be filmed by the MH team but did not mind being monitored by the Neurologist team in Sheffield provided she was given a takeaway. I said I am sure this could be arranged. Elizabeth would need to be closely monitored but this is essential. She said she would be happy to be monitored by experts in Sheffield . I am now extremely concerned that the MH team will try and send her to a supported living to avoid any pathological tests that need to be done because of the frequent fits. This must be determined first and foremost in a specialist hospital. Elizabeth has said on numerous occasions she does not wish to go into supported living which has been tried and totally failed before especially when she has an independent bungalow and even a two bed static caravan in the back garden. I am appalled and disgusted at what LPFT are doing when all along they should have taken a strong interest in her physical health and I am disclosing some interesting information below and the disturbing facts.
Subject: Neuroplasticity and Rapid Tranquillisation!
Neuroplasticity & Concomitant Drug ADRs:
Here are some potential explanations for the psychomotor ‘episodes’ Elizabeth has been experiencing.
The reason the episodes are getting more frequent is explained below. The frequency of the PRN is so short that the previous dose has not fully metabolised before they give her another one.
There is also a possibility that the depot anti-psychotic medication concomitantly administered with rapid tranquillisation is causing psychomotor dysfunction.
Chronic treatment with antipsychotic medications like Clopixol has been associated with alterations in brain structure and neuroplasticity, including changes in grey matter volume, dendritic spine density, and synaptic connectivity.
Benzodiazepines have also been shown to influence synaptic plasticity, albeit through different mechanisms.
The concomitant use of Clopixol and benzodiazepines may potentially interact to modulate neuroplasticity.
Chronic benzodiazepine use, such as repeated PRN rapid tranquillisation may be associated with alterations in brain structure and function. These changes may include reductions in grey matter volume, alterations in neurotransmitter systems, and neuroplastic changes. Neuroplastic changes will show up on a 3 Tesla MRI scanner. Presumably that is why certain people might not want such a scan done.
Neuroplastic changes can be detected using a 3 Tesla magnetic resonance imaging (MRI) scanner. A 3 Tesla MRI scanner is a powerful imaging tool that provides high-resolution images of the brain and has become the standard in clinical and research settings for studying brain structure and function.
Neuroplasticity refers to the brain’s ability to reorganize and adapt in response to experiences, learning, and environmental stimuli. These changes can occur at various levels, including alterations in synaptic connectivity, changes in neuronal morphology, and modifications in functional connectivity between brain regions.
With advanced imaging techniques such as functional MRI (fMRI), diffusion tensor imaging (DTI), and structural MRI, researchers and clinicians can visualize and quantify neuroplastic changes in the brain.
Here are a few examples of how neuroplasticity can be observed using a 3 Tesla MRI scanner:
1. Functional MRI (fMRI): fMRI measures changes in blood flow and oxygenation levels in the brain, which reflect neuronal activity. By analysing fMRI data, researchers can identify changes in brain activation patterns associated with learning, memory, and other cognitive processes, providing insights into neuroplasticity.
2. Structural MRI: Structural MRI techniques can detect changes in brain structure, including alterations in grey matter volume, cortical thickness, and white matter integrity. These changes may result from neuroplastic processes such as dendritic growth, synaptogenesis, and myelination, which can be visualized and quantified using high-resolution structural MRI scans.
3. Diffusion MRI (DTI): DTI measures the diffusion of water molecules in brain tissue and provides information about the microstructural organization of white matter pathways. By analysing DTI data, researchers can map changes in white matter integrity, such as alterations in fibre density, orientation, and connectivity, which are indicative of neuroplastic changes in the brain.
Overall, a 3 Tesla MRI scanner is capable of detecting and characterising neuroplastic changes in the brain, providing valuable insights into the mechanisms underlying learning, memory, recovery from injury, and adaptation to environmental stimuli. These imaging techniques play a crucial role in advancing our understanding of neuroplasticity and its implications for brain health and function.
Repeated rapid tranquilization with benzodiazepines can potentially lead to psychomotor dysfunction, although the likelihood and severity of this side effect may vary depending on factors such as the specific benzodiazepine used, the dosage, frequency of administration, individual susceptibility, and concurrent use of other medications.
Psychomotor dysfunction refers to impairments in motor coordination, reaction time, and cognitive function, which can manifest as symptoms such as drowsiness, dizziness, confusion, ataxia (loss of coordination), and impaired judgment. (this is what they mean by episodes) Benzodiazepines exert their effects on the central nervous system by enhancing the activity of the neurotransmitter gamma-aminobutyric acid (GABA), which can lead to sedation and relaxation.
During rapid tranquilisation, benzodiazepines are often administered to quickly alleviate acute agitation, aggression, or psychosis in emergency situations. While benzodiazepines can effectively reduce agitation and aggression, they can also cause sedation and other central nervous system depressant effects, particularly at higher doses or with rapid administration.
Repeated administration of benzodiazepines for rapid tranquilization may increase the risk of cumulative sedation and psychomotor dysfunction, especially if doses are given close together or if there is insufficient time for the drug to be metabolized and eliminated from the body between administrations. Additionally, certain factors such as age, medical conditions, and concurrent use of other medications may increase the susceptibility to benzodiazepine-induced psychomotor dysfunction.
Metabolism of benzodiazepines primarily occurs in the liver, where they undergo hepatic biotransformation mediated by various cytochrome P450 (CYP) enzymes, particularly CYP3A4, CYP2C19, and CYP2D6. Endocrine dysfunctions can affect the activity of these metabolic enzymes through various mechanisms, potentially leading to alterations in benzodiazepine metabolism.
It is essential for healthcare providers to carefully monitor patients who receive repeated rapid tranquilization with benzodiazepines for signs of psychomotor dysfunction and to adjust treatment accordingly to minimize the risk of adverse effects. Alternative strategies for managing agitation and aggression should also be considered, and the use of benzodiazepines should be limited to situations where the benefits outweigh the potential risks.
There is evidence to suggest that chronic benzodiazepine use may be associated with alterations in synaptic plasticity, which refers to the ability of synapses to strengthen or weaken over time in response to activity. Chronic benzodiazepine use has been shown to lead to changes in neurotransmitter systems, including alterations in GABA receptor expression and function, as well as changes in the density and morphology of dendritic spines, the small protrusions on neurons where synapses form.
These changes in synaptic plasticity may have implications for neuronal connectivity and brain function, although the extent to which benzodiazepines directly disrupt synaptic connectivity is not fully understood. Additionally, the clinical significance of these changes in synaptic plasticity in relation to the therapeutic effects and potential side effects of benzodiazepine use requires further investigation.
The increase in the frequency of the episodes you describe could indicate a condition known as dopamine supersensitivity psychosis. This is seen both with typical and atypical antipsychotics. The prolonged use of anti-psychotics that are not working due to her inability to metabolise anti-psychotics gives rise for concern. Has it not crossed anyone’s mind in that ‘treatment team’ that in spite of being on Clopixol for years she has not shown any sign of it being efficacious.
Since Elizabeth has never fully responded to the anti-psychotic medication they give her and they use PRN benzodiazepines for rapid tranquillisation far too frequently it is not surprising that she is having psychomotor problems. In effect this is another form of TD. If she is supersensitive then any dopamine antagonist could very well be causing this ADR.
A high resolution scan will indicate inflammation in the meso-limbic pathway affecting the dopamine receptors. The 1.5 Tesla scanner does not have sufficient resolution to do this. Inflammation can cause psychomotor problems as well as psychotic symptoms. Perhaps if they took the time to look for this specific adverse reaction they might not conclude the rather odd idea that the scan is normal.
By the way, the information I have on this is from The British Journal of Psychopharmacology just in case LPFT decide to dismiss this also.
Why 3T is necessary for detecting lesions
· ■ In more than 500 follow-up images, only four of 1996 new or enlarged multiple sclerosis lesions would have been missed with 3.0-T MRI without the administration of contrast material.
· ■ With 3.0-T MRI, the assessment of interval progression did not differ between contrast-enhanced and nonenhanced images.
Introduction
Inflammatory lesions in multiple sclerosis (MS) are detected as focal areas of high signal intensity on T2-weighted MR images. By depicting newly occurring lesions, MRI reveals subclinical disease activity. Therefore, regular follow-up MRI is considered a mainstay of clinical care for patients with MS or clinically isolated syndromes.
Earlier studies have reported that the administration of contrast material is necessary to maximize sensitivity for detecting new lesions. However, these results date back more than 2 decades and were based on two-dimensional images obtained with 4–5-mm-thick sections at magnetic field strengths of 1.5 T and lower.
MRI units with higher field strengths have become widely available, especially for brain imaging. In addition, three-dimensional isotropic MRI sequences were introduced and were shown to outperform conventional two-dimensional sequences in lesion depiction; they are therefore part of recommended MRI standards in MS . Furthermore, the double inversion-recovery (DIR) sequence was introduced. Although this sequence is best known for its ability to depict cortical lesions, it is also useful for depicting white matter lesions Recently, longitudinal subtraction techniques have been developed that show new or enlarged lesions as bright spots while pre-existing lesions and normal-appearing brain parenchyma are canceled out.* Such techniques substantially improve the sensitivity in the detection of new or enlarged lesions in MS at follow-up imaging.
We hypothesized that the use of contrast material does not improve sensitivity in the detection of new or enlarged lesions at follow-up MRI when modern three-dimensional sequences performed at a field strength of 3.0 T are used together with longitudinal subtraction maps. We therefore performed this study to investigate whether the use of contrast material has an effect on the detection of new or enlarged MS lesions and, consequently, the assessment of interval progression.
*The private 3T scans are much more able to see the lesions that the inappropriate 1.5T scanner cannot see.
The higher resolution scans cancel out the distortions and signal noise that hide the lesion and make the scan look normal.
1.5T MRI scanners are not fit for purpose in discovering brain lesions and inflammation.
Brain lesions and inflammation, especially in the temporal lobe are responsible for poor drug response and in some cases for diagnosis.
1.5T scans are responsible for false negative (normal) brain images.
EXAMPLE OF MISDIAGNOSIS
A woman who was told she had anxiety was later diagnosed with Autoimmune Basal Ganglia Encephalitis, a rare brain condition.
When Evie Meg, 23, was a teenager, she began to suffer bouts of panic and psychosis, and was diagnosed with anxiety disorder by doctors.
Meg began experiencing seizures when she was 17, along with temporary limb paralysis that left her unable to walk for a month, but was still told that it was due to anxiety.
Frustrated with the diagnosis, the then-teenager began sharing her symptoms and experiences on TikTok, where she was reached out to by a concerned follower.
“I posted a video of me walking across my kitchen without crutches, just taking a few steps,” Meg explains. “That video went viral and the support from it was amazing. People were saying how proud they were that I’d learnt to walk again. It just went from there, really.
“In 2021, I started getting loads of messages from this girl who had been commenting on all of my TikTok videos, saying I should look into this condition. She had it and she was so convinced that I had it.”
Because of this interaction, Meg booked in to see a specialist who diagnosed her with the brain inflammation disorder.
“When I got the diagnosis, we’d had to go private to find a specialist,” Meg says. “The NHS just don’t know what to do with me, because it’s such a complex and unusual condition.
“I have daily seizure activity. I have really severe pain above my right eye, and I haven’t been able to walk properly since May 2023. I get a lot of tiredness. It affects my mood quite a lot as well, I can get really upset or angry for no reason.”
Meg says she was put on antibiotics and steroids upon diagnosis, which stopped her seizures.
“It was crazy how quickly things turned around. I couldn’t believe it,” she adds. “We stayed with the doctors in London for a while, but I started becoming resistant to the antibiotics.
“Because my condition was not diagnosed for such a long time, it was allowed to progress and get a lot worse. It means it’s much more difficult to treat now, so we had to look for more intense options.”
Meg adds that her mum began researching the infusions that she needed and found a clinic in Poland that offered them – but at at £20,000 price tag.
“Last year, when I went to Poland for tests, they found loads of other infections in my blood, which could be causing the brain inflammation,” she adds.
“The SOT I had in January was to treat one of the infections, but we’re very early days – we’ve got to treat each one individually. Because they found so many, they have to do it multiple times to treat each infection. The next year or so for me is looking like a lot more SOT infusions – but I’m taking it one day at a time.”
Meg and her family have begun a fundraising campaign to help her have the treatment she needs, and have raised over £16,000 so far.
“The support has been pretty insane,” she says. “We had a local fundraiser in a church hall, and we raised over £4,000 just doing tombolas and raffles in that one afternoon.
“It’s been incredible – very overwhelming but in the best way. I became a lot more passionate about raising awareness when I got my correct diagnosis, because it just showed how it can be missed so easily. I really want people to know that and see that so that other people don’t go through what I did.”
Autoimmune Basal Ganglia Encephalitis is estimated to affect just 1.5 in every 100,000 people in England, and is characterised by the rapid development of akinesia, rigidity, and tremors.
It is a form of Encephalitis, which the NHS says is “an uncommon but serious condition in which the brain becomes inflamed”. The very young and the very old are the age groups most at risk.
Some symptoms of Encephalitis include seizures and fits, confusion, disorientation, changes in personality or behaviour, difficulty speaking, and weakness or loss of movement in parts of the body. It adds that causes are not always clear but, rarely, it can be caused by common viruses such as herpes simplex (cold sores), or chickenpox spreading to the brain; a problem with the immune system; or bacterial or fungal infections. And in Elizabeth’s case she contracted Covid twice at Ash Villa.
It is possible for some people to make a full recovery from Encephalitis, but the NHS says this can be a ‘long and frustrating’ process.
Additional reporting by SWNS.
Antipsychotics and the brain Neuro-imaging research (MRI scans) of the brains of people under psychosis reveal changes in brain activity. Some of these changes may be linked to the psychosis vulnerability itself (or to environmental risk factors that increase psychosis vulnerability, such as trauma), but many of these changes are clearly also related to several non-specific, external, factors, such as antipsychotics, smoking, obesity and drug use.
Animal tests have confirmed that antipsychotics indeed contribute to changes in the brain. The question remains, however, whether the changes in the brain caused by antipsychotics can also be linked to the specific risks. Also unknown is in how far these effects are permanent.
Antipsychotics and negative symptoms Antipsychotics work by making people somewhat indifferent. This lowers the ‘importance’ or ‘significance’ of their psychosis, sometimes to the point where the symptoms fade away completely. The problem is, however, that this medicine-induced indifference does not only affect the psychosis, but every personal emotion or experience. The suppressing of emotions makes the user of antipsychotics more numb and less active. The extent to which this happens is different from person to person, but some are seriously impaired by it.
This indifference is also called ‘secondary negative symptoms’. That term is confusing however, because it is impossible to make a distinction between the primary symptoms (caused by psychosis) and the secondary symptoms (caused by the antipsychotics).
In practice, the rule should be: negative symptoms (indifference, inaction) must be attributed to the antipsychotics unless proven otherwise. In other words: these symptoms require treatment, and should not be regarded as a consequence of psychosis when the real cause is the medication.
Can antipsychotics make psychosis worse? Dopamine supersensitivity syndrome (DPS) When taking antipsychotics over a long time, the body will try to compensate the effects of the medication. Because antipsychotics work by blocking the dopamine receptor D2 in the brain, the body responds by trying to remove this blockade some way or another. As early as in the 1960’s, the scientist Chouinard described how this can cause “supersensitivity” in the dopamine D2 receptor. As such, the eventual effect can be an increase of psychosis sensitivity instead of the expected decrease.
Symptoms of dopamine supersensitivity syndrome: Abnormal movements – also called tardive dyskinesia Increased psychosis vulnerability Increase of the dosage required to suppress psychosis More psychotic symptoms after stressful events.
Although the existence of DPS is not yet proven beyond doubt, it has become an issue of growing importance in practice. Some studies suggest that people who reduce medication, or quit altogether, have a higher risk of relapsing into psychosis in the first years (possibly due to the now ‘supersensitive’ D2 receptor). Yet on the longer term (when the ‘supersensitive’ receptor has returned to normal), they are better off than people who remain on their regular high dose.
Many psychiatrists are still unfamiliar with DPS It is important to recognise DPS in an early stage. Otherwise people can end up with huge doses of antipsychotics, while still only highly increasing the risk of psychosis. T.
Conclusion: antipsychotics and dopamine The perspectives on antipsychotics are rapidly changing. Anyone using antipsychotics, should in any case take the risk of DPS into account. Doctors prescribing antipsychotics should do the same. From the very first start of using antipsychotics, an accompanying strategy is required for reducing the dosage to its minimum, out of concern for the physical health and the effects on the brain. Sound alternatives are dopamine receptor partial agonists.
It is so disturbing the way the MH try to avoid essential scans and dismiss cancer and other neurological conditions without looking into it. Another shocking area is Enfield and also I am in touch with shocking cases in Weston – both areas only have a 1.5 Tesla by the way.
From: susan bevis Sent: 29 February 2024 12:38 To: CARECONCERNS (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST) <lpft.careconcerns@nhs.net> Cc: NEUROLOGYSECRETARIESLINCOLN (UNITED LINCOLNSHIRE HOSPITALS NHS TRUST) <ulh.tr-neurologysecs.lincoln@nhs.net>; Christopher Reid <Chris.Reid@parliament.uk>; Enquiries <Enquiries@cqc.org.uk>; CONNERY, Sarah (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST) <sarah.connery@nhs.net>
Subject: Re: EB – Update
I wish to address the serious threats made verbally by Dr WK.
“I am banning you indefinitely for inciting your daughter to attack members of staff on Xmas Day“. I want an apology for that for a start.
You have no right to take away the phone we as a family pay a contract. The matter of human rights will be address before the High Court. You are in breach of Art 8, 5, 3, Equality Act and the Code of Conduct for the MHA / MCA. Staff are acting ultra vires and you are treating my daughter like a restricted prisoner under the MHA 1983. What you are doing is entirely unlawful.
The restrictions you claim to have ended are very much continuing. You have no right to treat my daughter the way you are doing in the most degrading manner against all codes of conduct and the files will be requested by the court including all the notes being written behind my back by healthcare assistants who have been instructed to.
You are not using proper diagnostic scale PANSS and there is no proper scanner only a 1.5 Tesla and I am going to all the newspapers and TV stations to advise as this has cost someone their life before more lives are lost and Elizabeth will need to go to Sheffield to be re-tested under ultrasound for the cancer scare she had at Ash Villa since a Tesla 1.5 will not detect everything.
You had no right to ban the visits and now I want those comments made by Dr K and threats said to me verbally addressed and an apology. I will continue to issue invoices because you are depriving my daughter of her phone so that she cannot play her music and readily have contact therefore LPFT are guilty of discrimination. I will need all your reports Into your investigation of the alleged incident where Police were called on Xmas Day and to know that staff themselves who reported “concerns” have completed a Section 9 statement as we did. I have contacted the NMC who are taking my complaint very seriously as nursing staff are in breach of their own code of conduct but acting on instructions from a combination of Management, Clinical Lead and of course the person with ultimate control Responsible Clinician Dr Waqqas Khokhar who is acting ultra vires. Please do not assume Fridays as I am unable to visit on set days of the week.
You are acting totally unlawfully.
Yours faithfully
Susan A Bevis
Mother POA and Litigation Friend.
From: CARECONCERNS (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST) <lpft.careconcerns@nhs.net> Sent: 29 February 2024 12:17 To: susanb Subject: LB – Update
Dear Mrs Bevis,
We would like to communicate the following –
Ward round for E is at 12pm tomorrow, 1st March 2024. The clinical staff involved in E’s care would like for you to attend, specifically to discuss the filming of E’s episodes of distress to allow for further investigation of this with ULHT staff.
To address your recent concerns around E’s access to her mobile phone, E’s phone access was limited for a fixed period of time as part of a comprehensive care plan that considered E’s human rights. This was to ensure the response to her phone use did not adversely impact her engagement with, or the efficacy of, her treatment plan. This was ceased on Monday 5th February 2024 following a review of all of the relevant factors. To clarify this further, E’s phone is kept securely by ward staff, but E is able to request to use her phone at any time. In addition, ward staff regularly encourage E to use her phone to maintain contact with family.
Please be advised following your recent visit to Castle Ward that supervised visits to Castle Ward will be facilitated once a week, for one hour at a time. To request a time slot for visitation, please email the care concerns inbox. The inbox will confirm the date and time for the following week’s visit each Friday. All visits must be pre-arranged.
Kind regards,
The Mental Health Act Team.
Damning reports on patient care attached. One states that “patient neglect is a breach of the most fundamental medical ethics of all ‘first do no harm’.
LPFT have denied Elizabeth the medical ethic of autonomy and benificence by not getting her fully examined and monitored.
Their obsession with what she might be telling me at the expense of her care is a gross breach of the most fundamental of all the Principalist ethics of Beauchamp & Childress.
Here are examples of abuse from both Enfield and Lincolnshire:
My daughter was abused in the former area under both hospitals and supported living which is why I moved as I wanted her to be in the right environment like I provided briefly under and to give her a fresh start in what I thought was the right environment. I had challenged care in the community in a supported living scheme where things went wrong. There was no honesty and no rectification of anything in the circumstances. Everything stemmed from there onwards. Elizabeth had been subject to institutional care on and off where not once when things went wrong did anyone raise their hands.
The Discharge Note stated “Abnormal Findings on Scan pointing to CNS twice. I have not been unable to get an explanation?
Upon moving we have been subject to extreme bullying because I have continually asked what the scans meant done by former area. When I discovered Dr Shahpasandy of Ash Villa did some fantastic research on the Limbic System I asked if Elizabeth could be included. I was then faced with no end of excuses. It was as though none of these doctors (Psychiatrists) wanted her to have the research that discovered that a former patient did not in fact have schizophrenia but inflammation of the brain and needed a different form of treatment and as a result of that became better. That is all I have ever wanted for my daughter to be properly pathologically tests since according to past file copies, it clearly says “Anterior Region Medial Temporal Compromise and so I checked what this meant and I was told “well done” by Headways that MH professionals training did not go nearly far enough to be able to conclude on neurological conditions, she was a former MH nurse. This puts into question the training for a start and that why isn’t training under MH more comprehensive and that it should in fact go much further in order that patients are not dismissed for underlying physical health conditions that may need a different kind of medical treatment.
Because I have dared to question I have been subject to bullying – extreme bullying. I was told “I am displacing you as NR” I thought not again as I have had a lifetime of this kind of treatment. It would appear all you have to do is to challenge in order to be the subject of bullying and various people including carers and former patients have tried to advise me that I should go along with everything but how can I when people are dying from being misdiagnosed and not having the right kind of treatment because the NHS is failing to look properly into neurological and underlying physical health conditions which could be autoimmune, could be endocrine dysfunction, thyroid, infection. It is very wrong to give someone a label for life and not be open to consider that there may be underlying physical health factors that need proper investigation.
Just now I have been on the phone to Ron Coleman. Both he and Karen Taylor through “Working-to-recovery provided wonderful care at their home on the Isle of Lewis. This care took my daughter to Spain and all over France and then to Australia, the account of this is on the Rightful Lives Website. She was in a terrible state before going away but came home unrecognisable. I will be forever grateful to Working-to-Recovery and thanked Ron Coleman for his wonderful care today and how the entire family took my daughter to the most wonderful locations and tried to work properly with her for the first time ever UNLIKE THE NHS. Unfortunately the NHS is rife with bullying and what I am finding right now is that staff are acting ultra vires. When my daughter returned home from Australia she wanted a job, she was totally unrecognisable as she had psychotherapy but because my shocking area of Enfield provided nothing she went downhill again. How I wish she had stayed forever in Australia. If I never saw my daughter again I would be happy in the knowledge she was in the right company and environment.
Via the NHS I have been described as someone who is controlling, abusive, aggressive – a vile person. I am not going to defend myself. I will leave it to my readers to decide.
Via the NHS upon moving I have been subject to severe bullying as follows:
First of all they declined to get the treatment up and running which was the clopixol depot leading to her going downhill – even I as just a mother knows that you cannot just stop these powerful drugs in one go.
Secondly they wanted the POA so they tried to make me look abusive – psychological abuse was mentioned. The Public Guardian Office had to investigate and found in my favour.
Thirdly they wanted the role of NR to be given to the social services, a conflict of interest. There followed months and months of litigation where I desperately tried to defend myself but there was no hope under this court because judges do not have the remit to challenge whether someone is really suitable or not. I was threatened constantly with costs as a result. That is known as SLAPPS.
“Suitability” should surely be a parent and carer who visits regularly and who cares. I have no say in anything in terms of treatment as this comes under doctors however I have gone by past file records. I have reports from other doctors who thoroughly dispute the diagnosis and I have noticed how Elizabeth has not been listened to so have done what any parent would do and stick up for her – defend her which has not made me popular. However no-one can dispute the fact that I have tried to help giving everything I have got to my disabled daughter and not expecting anything in return apart from the continuation of the former area’s medication whether I agreed with it or not. It is not that I am saying no-one else cares in the family but I happen to live the closest plus visit weekly. Anyway, the County Court Displaced me and all I will say is noone has effectively acted as NR and social services in any case are “a conflict of interest” and have done nothing to safeguard my daughter during the time at Ash Villa.
Anyway because I dared to challenge I was treated in the same way as present previously at Ash Villa:
phone restricted and visiting 2-1. No leave for months and months on end. Several flawed capacity assessments done not taking into account Principle 4, accident leading to possible injury and the start of the “epileptic fits” which noone knows really what is the cause. Today I have been asked whether Elizabeth agrees to be filmed during an episode. She disagreed. So what now? I personally think she needs to be assessed properly in Sheffield as an inpatient on a neurological ward and where they have the correct scanner ie a Tesla 3.
I am making everyone aware that there is a need for a Tesla 3 scanner at Lincs because a 1.5 does not pick everything up and has been known to miss tumours. All I want is an explanation of what is show on the MRI scans in certain images.
The treatment has been awful for my daughter. She is already held a prisoner but imagine how this would feel when denied basic human rights and proper pathological tests.
She has been treated in a degrading manner for far too long with phone taken away, visits restricted and medical pathological tests flatly refused.
I will add to this blog later to describe what treatment is given to patients under LPFT
Reader and Gillespie BMC Health Services Research 2013, 13:156
R E S EAR CH A R TIC L E
Patient neglect in healthcare institutions: a systematic review and conceptual model
Tom W Reader* and Alex Gillespie Abstract Background: Patient neglect is an issue of increasing public concern in Europe and North America, yet remains poorly understood. This is the first systematic review on the nature, frequency and causes of patient neglect as distinct from patient safety topics such as medical error. Method: The Pubmed, Science Direct, and Medline databases were searched in order to identify research studies investigating patient neglect. Ten articles and four government reports met the inclusion criteria of reporting primary data on the occurrence or causes of patient neglect. Qualitative and quantitative data extraction investigated:
(1) the definition of patient neglect,
(2) the forms of behaviour associated with neglect,
(3) the reported frequency of neglect, and
(4) the causes of neglect. Results: Patient neglect is found to have two aspects. First, procedure neglect, which refers to failures of healthcare staff to achieve objective standards of care. Second, caring neglect, which refers to behaviours that lead patients and observers to believe that staff have uncaring attitudes. The perceived frequency of neglectful behaviour varies by observer. Patients and their family members are more likely to report neglect than healthcare staff, and nurses are more likely to report on the neglectful behaviours of other nurses than on their own behaviour. The causes of patient neglect frequently relate to organisational factors (e.g. high workloads that constrain the behaviours of healthcare staff, burnout), and the relationship between carers and patients. Conclusion: A social psychology-based conceptual model is developed to explain the occurrence and nature of patient neglect. This model will facilitate investigations of
i) differences between patients and healthcare staff in how they perceive neglect,
ii) the association with patient neglect and health outcomes,
iii) the relative importance of system and organisational factors in causing neglect, and
iv) the design of interventions and health policy to reduce patient neglect. Keywords: Neglect, Patient safety, Caring, Organisational culture, Systematic review Background Patient neglect, defined as “the failure of a designated care giver to meet the needs of a dependent”
1, has become an issue of concern in both North America and Europe
[2,3]. In the UK, this has been driven by media outlets
[4,5], charities
[6], and health regulators [7]. Headlines such as “Want to know the NHS’s real problem? Ask a nurse for a bowl of cornflakes”
[8], “Shamed hospital accused of leaving dying patients to starve”
[9], and “Can patient neglect be a violation of human rights?”
[10] capture concerns relating to patient neglect. They reflect public anxiety, with patients and families making 22,845 complaints to the NHS in 2011on issues relating to staff attitudes, communication, and patient dignity
[11]. Senior politicians acknowledge the issue, and argue that neglect has been “hidden away” [12] and that healthcare institutions must ensure “every patient is cared for with compassion and dignity”
[13].Solutions include “reducing stifling bureaucracy” [14], ensuring nursing staff talk to patients at least “once an hour” [13], utilising legislation and regulation to ensure staff consider patient’ “wellbeing and dignity”
[15], and making staff sign-up to a “code of conduct” on dignity and respect
Doing No Harm: Enabling, Enacting, and Elaborating a Culture of Safety in Health Care Author(s): Timothy J. Vogus, Kathleen M. Sutcliffe and Karl E. Weick Source: Academy of Management Perspectives , November 2010, Vol. 24, No. 4 (November 2010), pp. 60-77 Published by: Academy of Management Stable URL: https://www.jstor.org/stable/29764991 JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range of content in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new forms of scholarship. For more information about JSTOR, please contact support@jstor.org. Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at https://about.jstor.org/terms Academy of Management is collaborating with JSTOR to digitize, preserve and extend access to Academy of Management Perspectives ARTICLES Doing No Harm: Enabling, Enacting, and Elaborating a Culture of Safety in Health Care by Timothy J. Vogus, Kathleen M. Sutcliffe, and Karl E. Weick
Academy of Management is collaborating with JSTOR to digitize, preserve and extend access to Academy of Management Perspectives This content downloaded from https://www.jstor.org/stable/29764991
Published by: Academy of Management Stable URL: https://www.jstor.org/stable/29764991 Executive Overview Medical error has reached epidemic proportions, and researchers have developed insufficiently sophisticated models of safety culture to match the complexity of the challenge of safety in health care. This has left providers and researchers with an inadequate conceptual toolkit for improving safety. To rectify the resulting crisis we consolidate fragments of management research into a comprehensive and integrative framework of how patient safety is produced and sustained through safety culture. Safety culture involves actions that single out and focus safety-relevant premises and cultural practices that reduce harm. This entails (a) enabling, which consolidates the premises for a safety culture; (b) enacting, which translates consolidated premises into concrete practices that prioritize safety; and (c) elaborating, which enlarges and refines the consolidation and translation. We close by discussing the implications of our framework for future research on key issues such as efficiency-safety trade-offs, interactions among components of the framework, and feedback loops. In the face of competing priorities (e.g., efficiency), organizations often inadequately prioritize safety relative to other goals (Perrow, 1984)* Although safety challenges plague many industries, the problem is especially acute in health care. Health care presents a challenging paradox by pairing the mandate to “do no harm” with mounting evidence that much harm is done in the course of delivering care. In 1999 the Institute of Medicine (IOM) released a report titled To Err Is Human, in which medical error was citedas the eighth leading cause of death in the United States (more than motor vehicle accidents, breast cancer, or AIDS), responsible for as many as 98,000 deaths annually (IOM, 1999). A 2002 report by the Centers for Disease Control (CDC) stated that almost 2 million Americans acquire infections in the hospital, contributing to those 98,000 deaths each year. More specifically, 48,600 central-line bloodstream infections occur annu? ally, with one third of those patients dying (Buerhaus, 2007). Additionally, an estimated 2% to 4% of patients (between 670,000 and 1.3 million) fall during their hospitalization in the United States annually, with 2% to 6% of those falls (13,000 to 78,000) resulting in injury. In sum, as many as 88 people out of every 1,000 will suffer injury or Timothy J. Vogus (timothy.vogus@owen.vanderbilt.edu) is Assistant Professor of Management at the Owen Graduate School of Management, Vanderbilt University. Kathleen M. Sutcliffe (ksutclif@umich.edu) is the Gilbert and Ruth Whitaker Professor of Management and Organizations at the Stephen M. Ross School of Business, University of Michigan. Karl E. Weick (karlw@umich.edu) is the Rensis Likert Distinguished University Professor of Organizational Behavior and Psychology at the Stephen M. Ross School of Business, University of Michigan. Copyright by the Academy of Management; all rights reserved. Contents may not be copied, e-mailed, posted to a listserv, or otherwise transmitted without the copyright holder’s express written permission. Users may print, download, or e-mail articles for individual use only. We would like to thank AMP Editor Garry Bruton, Peter Cappelli, Ranga Ramanujam, Jen Vogus, and two anonymous reviewers for thoughtful and constructive comments that substantially improved the quality and contribution of this manuscript. We also thank Aidan Vogus for helping us see the importance of this work.
I have already revealed Elizabeth’s scans which were done in November at Lincoln County Hospital with the result of “normal”. I would urge all of my readers to double check what scanner has been used as a 1.5 scanner has not picked up what is clearly visible on the private scans I had done through S G Radiology. I am waiting for an explanation as to what the images portray as I cannot accept these images to be normal. They even state “trauma” so as a parent or carer it is evident that you cannot always assume that normal means normal. A while back Elizabeth had an ultrasound as there were fears of cancer. Now I want all the scans done again under a Tesla 3. I have heard a Tesla 7 is even better and will look into where this can be done in the UK. So Lincolnshire, Enfield, Weston are just three examples where they do not have the up to date scanner and therefore you cannot rely on the results. This affects not just people under MH but everyone.
For so long now I have been trying to get answers – it clearly states “Anterior Region Medial Temperol Compromise which is not a mental illness and yet Elizabeth has been treated under MH with massive dosage of antipsychotics that do not work and is “treatment resistant” – poor/non metaboliser which I have prove by P450 tests. Now everything is falling into place and it is something I want to share with all of you especially those going through cancer treatment. Never trust the word “normal” and check what scanner your Trust has. I am currently asking my MP, Victoria Atkins why Lincolnshire does not have a scanner that is reliable. This means all of Elizabeth’s treatment may be affected as last year there was a cancer scare. Now I want all the scans/ultrasounds done through Sheffield and for Elizabeth to be referred to a Neurological Ward where for once her physical health can be properly assessed over a period of weeks. If the MH team stand in my daughter’s way of her physical health appointments and pathological tests I will report everything on here. I have already requested reports from all the professional bodies who have done nothing so far to stop the abuse to my daughter. Most importantly doctors should put the physical health of their patients first and foremost. I have now highlighted how patients are being deprived under just one area and how patients could have lost their lives due to the scans and how patients under the MH are refused pathological tests. This is why I was banned for months on end visiting my daughter and bullied by various doctors and this needs to be looked into. Police time has been wasted. Having lost close friends to cancer I intend to give this massive publicity.
LPFT under MH do not use PANSS??? Below is what I have written to Lincolnshire Partnership Trust as I am concerned for all the patients on Castle and Ellis Ward who may not have had reliable scans and I do not think anyone is being treated properly and wish to share so that everyone can be aware of the true facts:
PANSS
The PANSS score is an essential diagnostic tool which LPFT are not using and should be. All the scans may need to be re-done under scanners in Sheffield not just the MRI – everything and you may have to review all the patients on both Castle and Ellis Wards who have had scans done in Lincoln under the 1.5 Tesla in light of the revelations below.
The PANSS score is a long established test approved by the Royal College of Psychiatrists and used by NHS Mental Health Teams in many of the trusts to determine the severity of the schizophrenia the patient is suffering from. Its purpose is to confirm diagnosis, to guide the treatment regimen and to determine suitability for matters such as section 17 leave, suitability of the patient for post-discharge accommodation and eventual discharge from mental health care.
Here are LPFT’s comments below:
“LPFT does not use the PANSS scale for various reasons but does use the Glasgow Antipsychotic side effect scale (GASS). This measures the side effects of antipsychotics rather than the efficacy of antipsychotics”.
This is totally unsatisfactory for the following reasons. To begin with to quote LPFT’s own words “for various reasons” gives no explanation at all why this scale is not used by LPFT and is a cursory and unhelpful excuse.
The PANSS scale as mentioned above is crucial in determining not only treatment but deprivation of liberty and the ability of Elizabeth to enjoy leave and to have quality time off the ward. Elizabeth’s stifling detention without hope of even the chance to have a day out or to spend time with her family on important occasions like Christmas and her birthday are a contribution to her state of mind and a detriment to her eventual recovery.
The scale is also used to determine an appropriate treatment regimen which goes beyond the simple use or rapid tranquillisation and isolation preferred by the staff of the hospital in which she is detained. The hospital has obstructed all attempts to have Elizabeth’s mental health condition based on a determination that their ‘diagnosis ‘ of schizophrenia would be the only option. Elizabeth is now seeing a neurologist but that has only happened because that intervention was sought by me and was indeed actively discouraged and obstructed by the Responsible Clinician and the Clinical Lead on the ward.
The Glasgow Antipsychotic Side effect (GASS) scale that LPFT refer to in their email has an entirely different purpose to the PANSS scale and you are well aware of that. The GASS effect scale is for detecting adverse drug reactions and it has to be said if they are indeed using this they have ignored a number of these over the last two and a half years in spite of them being pointed out to them.
LPFT are fully aware that the GASS scale is not a substitute for PANSS but an entirely different test and the reply to the NR was disingenuous and unhelpful. To date no detailed explanation of why PANSS is not being used has been given and the Mental Health Act Team (notably the email does not identify its author) have failed to help once again. Please explain.
In the absence of proper monitoring by the people entrusted with Elizabeth’s care is it hardly surprising that after two and a half years subjected to a deprivation of liberty regime more restrictive than a section 37/41 order and constant prn rapid tranquillisation that she has made no improvement and is as far away from discharge as she ever has been.
The fact is the private scans are most certainly more superior to theirs and have been shown to numerous experts who are biomedical scientists yet they agree. If LPFT hadn’t spent a fortune getting rid of me as NR they would have more money to spend on decent scanners such as Tesla 3 and not having one is putting everyone’s life at risk not just those under MH. The taking away of my daughter’s right of capacity and autonomy is the biggest violation of all human rights. About 10 doctors apart from Dr Memons of Cygnet have stood in the way of her having MRI scans so that is why I was suspicious and arranged it myself. The MH system is ridiculous and I was the best NR and they got rid of me for their own convenience which again is abrogation of my daughter’s human rights. As highlighted in Medscape it is mentioned about brain tumours being missed and metastacising before being found which is potentially fatal which is why I am warning everyone not to trust their NHS scans and to check on which scanner has been used by their Trust.
It is also important to get brain lipids tested. They can affect both metabolising enzymes and result in ADRs. Several endocrine/metabolising disorders are associated with elevated levels of lipids (hyperlipidemia).
RESPONSIBLE CLINICIANS ARE SUPPOSED TO FOLLOW THE MHA 1983 BUT UNDER LPFT WHAT IS BEING DONE IS NOT CONDUCIVE TO ELIZABETH’S RECOVERY AND I WILL FEATURE MORE SHOCKING REVELATIONS ON MY NEXT BLOG. THEY NEEDED TO ROB HER OF HER CAPACITY SO THAT THEY COULD ABUSE THE CONCEPT OF THERAPEUTIC NECESSITY WHILST LABELLED WITH NO CAPACITY. I HAVE CAUGHT ON TO THEIR CRAFTINESS AS THIS GETS THEM OUT OF CONSULTING WITH HER OR RECORDING HER WISHES AND THIS IS WHY THEY GOT RID OF ME AS NR AND THIS IS TO PROTECT THEMSELVES. NO HUMAN RIGHTS AT ALL ARE TAKEN INTO ACCOUT BY LPFT. THE TERRIBLE DENIAL OF LIFE EXPERIENCE IS DETRIMENTAL TO MY DAUGHTER’S MENTAL AND PHYSICAL HEALTH AND TOTAL ABROGATION OF MEDICAL ETHICS. EVEN A S37/41 PATIENT IS NOT DENIED SUCH RIGHTS. HOW CAN HER DETENTION BE LAWFUL UNDER MHA 1983. THEY CONTINUALLY FLOUT THE STATUTORY SAFEGUARDS. THEY SHOULD BE SUBJECTED TO JUDICIAL REVIEW AND PROFESSIONAL MISCONDUCT ACTIONS.
Why 3T is necessary for detecting lesions
■ In more than 500 follow-up images, only four of 1996 new or enlarged multiple sclerosis lesions would have been missed with 3.0-T MRI without the administration of contrast material.
■ With 3.0-T MRI, the assessment of interval progression did not differ between contrast-enhanced and nonenhanced images.
Introduction
Inflammatory lesions in multiple sclerosis (MS) are detected as focal areas of high signal intensity on T2-weighted MR images. By depicting newly occurring lesions, MRI reveals subclinical disease activity. Therefore, regular follow-up MRI is considered a mainstay of clinical care for patients with MS or clinically isolated syndromes.
Earlier studies have reported that the administration of contrast material is necessary to maximize sensitivity for detecting new lesions. However, these results date back more than 2 decades and were based on two-dimensional images obtained with 4–5-mm-thick sections at magnetic field strengths of 1.5 T and lower.
MRI units with higher field strengths have become widely available, especially for brain imaging. In addition, three-dimensional isotropic MRI sequences were introduced and were shown to outperform conventional two-dimensional sequences in lesion depiction; they are therefore part of recommended MRI standards in MS . Furthermore, the double inversion-recovery (DIR) sequence was introduced. Although this sequence is best known for its ability to depict cortical lesions, it is also useful for depicting white matter lesions Recently, longitudinal subtraction techniques have been developed that show new or enlarged lesions as bright spots while pre-existing lesions and normal-appearing brain parenchyma are canceled out.* Such techniques substantially improve the sensitivity in the detection of new or enlarged lesions in MS at follow-up imaging.
We hypothesized that the use of contrast material does not improve sensitivity in the detection of new or enlarged lesions at follow-up MRI when modern three-dimensional sequences performed at a field strength of 3.0 T are used together with longitudinal subtraction maps. We therefore performed this study to investigate whether the use of contrast material has an effect on the detection of new or enlarged MS lesions and, consequently, the assessment of interval progression.
*The private 3T scans are much more able to see the lesions that the inappropriate 1.5T scanner cannot see.
The higher resolution scans cancel out the distortions and signal noise that hide the lesion and make the scan look normal.
1.5T MRI scanners are not fit for purpose in discovering brain lesions and inflammation.
Brain lesions and inflammation, especially in the temporal lobe are responsible for poor drug response and in some cases for diagnosis.
1.5T scans are responsible for false negative (normal) brain images.
Neuro Second Opinion Catches Missed Brain Lesions Suggestive of MS
American Roentgen Ray Society Dynamic contrast-enhanced MRI (DCE-MRI) has clearly been shown to be a highly sensitive tool for the detection of breast cancer [1–14]. Reported high sensitivity (83– 100%) [1–5] of MRI for breast cancer led im[1]agers initially to presume that non-enhancing legions on MRI were benign and did not warrant biopsy [1, 15]. However, subsequently reported articles have shown that all malignant lesions do not show enhancement at DCE[1]MRI [2, 5, 16–20], with enhancement absent in up to 12% of known malignant lesions. In a recent multi-institutional study of 995 lesions in 854 women, Schnall et al. [20] reported that 16% of 77 ductal carcinoma in situ (DCIS) lesions and 3% of 422 invasive cancers showed no enhancement. Teifke et al. [18] found 28 (8.4%) of 334 invasive cancers and 13 (65%) of 20 non-invasive cancers were missed at MRI. The reasons given for lack of visualization of these missed lesions were technical difficulties, reader percep[1]Keywords: breast cancer, DCE-MRI, dynamic contrast-enhanced MRI DOI:10.2214/AJR.09.3568 Received September 3, 2009; accepted after revision December 8, 2009.
R. A. Schmidt is a minor stockholder in Hologic Inc., and his spouse receives grant support from Philips Healthcare. G. M. Newstead receives grant support from Philips Healthcare, and her spouse is a minor stockholder in Hologic Inc. WOMEN ’ S I M A G I N G OBJECTIVE.
The objective of our study was to determine the sensitivity of cancer detection at breast MRI using current imaging techniques and to evaluate the characteristics of lesions with false-negative examinations. MATERIALS AND METHODS. Two hundred seventeen patients with 222 newly diagnosed breast cancers or highly suspicious breast lesions that were subsequently shown to be malignant underwent breast MRI examinations for staging. Two breast imaging radiologists performed a consensus review of the breast MRI examinations. The absence of perceptible contrast enhancement at the expected site was considered to be a false-negative MRI. Histology of all lesions was reviewed by an experienced breast pathologist. RESULTS. Enhancement was observed in 213 (95.9%) of the 222 cancer lesions. Of the nine lesions without visible enhancement, two lesions were excluded because the entire tumor had been excised at percutaneous biopsy performed before the MRI examination and no residual tumor was noted on the final histology. The overall sensitivity of MRI for the known cancers was 96.8% (213/220); for invasive cancer, 98.3% (176/179); and for ductal carcinoma in situ, 90.2% (37/41). CONCLUSION.
In a population of 220 sequentially diagnosed breast cancer lesions, we found seven (3.2%) MRI-occult cancers, fewer than seen in other published studies. Small tumor size and diffuse parenchymal enhancement were the principal reasons for these false[1]negative results. Although the overall sensitivity of cancer detection was high (96.8%), it should be emphasized that a negative MRI should not influence the management of a lesion that appears to be of concern on physical examination or on other imaging techniques. Shimauchi et al. MRI-Occult Breast Cancers Women’s Imaging Original Report Downloaded from ajronline.org by 90.246.25.176 on 02/27/24 from IP address 90.246.25.176. Copyright ARRS. For personal use only; all rights reserved AJR:194, June 2010 1675 MRI-Occult Breast Cancers stitution. Forty-four lesions in 44 patients were excluded because the final pathology at lumpectomy or mastectomy was performed at other institutions and was not available for review by our pathologists. The remaining 222 cancers in 217 patients were the subject of this retrospective review. The patients ranged in age from 28 to 85 years (median, 58 years). The spectrum of malignancy size and histology in these 217 patients is shown in Table 1. Of the 222 cancers studied, 84 (37.8%) lesions were palpable, 80 (36.0%) lesions were non-palpable, and clinical data as to palpability was not available for 57 (25.7%) lesions; 209 (94.1%) lesions were visible at mammography, 10 (4.5%) lesions were not visible at mammography, and mammograms were not available for three (1.4%) lesions. Additionally, 166 (74.8%) lesions were visible at sonography, 16 (7.2%) lesions were not visible at sonography, and ultrasound images were not available for 40 (18.0%) lesions. All index cancers, except 32 of 222 lesions, had been diagnosed by percutaneous biopsy or fine-needle aspiration (FNA) before MRI. The remaining 32 cancers underwent MRI because other imaging and clinical findings suggested a highly suspicious lesion and subsequent tissue sampling proved malignancy. Conventional Diagnostic Imaging In all but three patients, mammograms (obtained with different equipment and films, many from different referral centers) were available and were reviewed at our institution by breast imaging specialist radiologists before MRI. Mammograms obtained at outside referral centers accounted for approximately 20% of the total 217 patients. All patients with invasive cancer or extensive DCIS lesions (166 cases, 75%) underwent target[1]ed ultrasound examination of the affected breast and the ipsilateral axillary region, using an ATL HDI 5000 unit (Philips Healthcare International) and a 5-12–MHz linear transducer, before MRI. These imaging examinations were performed by breast specialist radiologists at our institution. An additional ultrasound examination was not standard procedure for patients with a diagnosis of pure DCIS at our institution unless mammograms showed extensive disease suspicious for the presence of an invasive component. MRI Protocol MRI examinations were performed using two 1.5-T imaging units (Signa, GE Healthcare, for 116 patients; and Intera Achieva, Philips Healthcare, for 101 patients). All patients underwent MRI in the prone position using parallel imaging technique. A dedicated 8-channel breast coil was used for the Signa scanner, and a dedicated 7-channel breast coil was used for the Intera Achieva scanner. After obtaining bilateral non-fat-saturated T2-weighted images (TR/TE: Signa, 5,000/103.5; Intera Achieva, 16,907/120) of the breasts, a T1-weighted 3D gradient-echo sequence was performed before and 20 seconds after the injection of contrast material. For the Signa scanner, the imaging parameters were as follows: 4.6/2.2; flip angle, 10°; field of view (FOV), 34 × 34 cm; matrix, 320 × 320; section thickness, 2 mm; and acquisition time, 75 sec[1]onds. For the Intera Achieva scanner, the parameters were as follows: 7.9/3.9; flip angle, 10°; FOV, 48 × 48 cm; matrix, 352 × 352; section thickness, 2 mm; and acquisition time, 75 seconds. A dynamic study in the axial plane was performed six times after initiation of an IV injection of 0.1 mmol/kg of gadodiamide (Omniscan, GE Healthcare) at a rate of 2 mL/s, which was followed by a 20-mL saline flush at the rate of 2 mL/s. MRI examinations were processed by CADstream, version 4.1 (Confirma), and subtraction images, time course curves, and angiogenesis maps were obtained. The images were transferred to a workstation (Advantage Windows, software version 4.0, GE Healthcare) for analysis. Image Analysis IRB-approved retrospective review by consensus was performed by two radiologists with expertise in breast MRI, one with 15 years’ experience and the other with 5 years. Images were interpreted with the benefit of a brief clinical history, knowledge of the histopathologic findings, and knowledge of the mammography and sonography results. In addition to the original images, maximum-intensity-projection and multiplanar reconstruction images were reviewed. The reviewers called findings positive even when there was no color on angiogenesis maps or when, for example, there was a persistent type of curve; they relied on morphology for diagnosis in these cases because TABLE 1: Pathologic Diagnosis in 217 Patients With 222 Malignancies Diagnosis No. (%) of Malignant Lesions No. (%) of Malignant Lesions by Size < 2 cm 2–5 cm > 5 cm Not Available Invasive ductal carcinoma 160 (72) 94 (80) 54 (76) 11 (55) 0 (0) Invasive lobular carcinoma 19 (8) 8 (7) 9 (13) 2 (10) 0 (0) Ductal carcinoma in situ 44 (20) 15 (13) 8 (11) 7 (35) 14 (100) Total 222 (100) 117 (100) 71 (100) 20 (100) 14 (100) TABLE 2: False-Negative Lesions at Dynamic Contrast-Enhanced MRI Case No. Patient Age (y) Pathology Imaging Reason for False[1]Type of Cancer Nuclear Grade Size (mm) Mammography Sonography Size (mm) Negative MRI 1 46 Extensive DCIS 2 NA Pleomorphic and linear calcifications NA 30 Diffuse parenchymal enhancement 2 43 DCIS 3 30 Pleomorphic calcifications Negative 25 Diffuse parenchymal enhancement 3 54 Multifocal DCIS 3 NA Punctate calcifications NA 5 Unknown 4 79 DCIS 1 5 Pleomorphic calcifications NA 5 Small size 5 53 IDC with DCIS 3 IDC, 0.8; DCIS, 10 Amorphous calcifications NA 10 Unknown 6 49 IDC with extensive DCIS 2 IDC, 8; DCIS, NA Pleomorphic and linear calcifications Hypoechoic masses 65 Diffuse parenchymal enhancement 7 44 IDC with DCIS 2 IDC, 12; DCIS, NA Negative Mixed echogenic mass 10 Unknown; low-signal mass on T2-weighted images Median 46 10 Note—DCIS = ductal carcinoma in situ, IDC = invasive ductal carcinoma, NA = not applicable. Downloaded from ajronline.org by 90.246.25.176 on 02/27/24 from IP address 90.246.25.176. Copyright ARRS. For personal use only; all rights reserved 1676 AJR:194, June 2010 Shimauchi et al. some malignant lesions especially DCIS and in[1]vasive lobular carcinoma (ILC) lesions can show slow uptake and perceptible kinetics [21, 22]. The absence of perceptive contrast enhancement at the expected site of the lesion was considered to be a false-negative MRI. Each study was also evaluat[1]ed with bilateral breast parenchymal enhancement scores of minimal, mild, moderate, or marked enhancement by consensus opinion. Technical factors such as patient motion, poor fat suppression, or susceptibility artifacts caused by percutaneously placed metallic clips did not compromise any of the study data sets. Histopathologic Correlation Of the 222 malignant cases, mastectomy was performed for 92 (41%) cases and breast-conserving surgery lumpectomy, with or without needle localization guidance, was performed for 130 cas[1]es (59%). Histology results of all lesions were re[1]viewed by an experienced breast pathologist with 25 years of experience in breast pathology. Tumor type, grade, size, and histologic subtype were documented in the pathology reports. In general, in our pathology department, extensive DCIS is defined as a lesion larger than 5 cm. Correlation between imaging and pathology for each case with regard to location and size and treatment management decisions were discussed for each case at weekly inter[1]nal multidisciplinary breast conference. Results Of the 222 cancerous lesions, enhancement was observed in 213 lesions (95.9%). There were nine examinations that showed no enhancement on MRI. All nine patients had undergone core biopsy or FNA before the MRI examination. Two of the nine lesions were excluded from our false-negative analysis, both presented with a cluster of calcifications, because the entire tumor had been excised by stereotactic core biopsy performed before the MRI examination. In these cases, no residu[1]al tumor was noted at histology on the sub[1]sequent excised breast specimens. Histology of both lesions indicated low-grade DCIS. The sensitivity of MRI for the known cancers was, therefore, 96.8% (213/220) for all cancer, 98.3% (176/179) for invasive cancer, and 90.2% (37/41) for DCIS. Of the 217 patients, 35 patients (16.1%) were recalled for MRI-directed ultrasound, 22 patients (10.1%) underwent ultrasound biopsies with benign results, and nine patients (4.1%) underwent MRI biopsies with benign results. The seven (3.2%) nonenhancing cancers included four cases of DCIS (one low-grade, one intermediate-grade, two high-grade), and three cases of invasive ductal carcinoma (IDC) (two intermediate-grade, one high-grade), as shown in Table 2. One of the two scanners was used for 116 patients (119 lesions), and four malignant lesions (3.4%) were missed. The other scanner was used for 101 patients (103 lesions), and three lesions (2.9%) were missed. All of the false-negative lesions except one were detected at mammography. The mammographic features of these lesions were classified as pleomorphic and linear calcifications (2/6), pleomorphic calcifica[1]tions (2/6), amorphous calcifications (1/6), and punctate calcifications (1/6). One lesion was detected as a palpable, tender mass in the retroareolar region and was visible at sonog[1]raphy but not at mammography. The overall A C Fig. 1—79-year-old woman with history of right lumpectomy for ductal carcinoma in situ (DCIS) 10 years earlier (case 4 in Table 2). A, Craniocaudal magnification view of right breast from routine follow-up mammography shows 5-mm cluster of pleomorphic calcifications (arrow) near lumpectomy scar. Stereotactic core biopsy revealed DCIS, grade 1. B, Craniocaudal mammographic view of right breast obtained after biopsy shows metallic clip with a few residual calcifications (arrow) at site of biopsy. C, T2-weighted image shows susceptibility artifact from metallic clip (arrow). D, On early phase of dynamic contrast-enhanced study (subtraction, T1-weighted image), no enhancement is seen around clip (arrow). Subsequent right mastectomy revealed DCIS measuring 5 mm in vicinity of biopsy site. B D Downloaded from ajronline.org by 90.246.25.176 on 02/27/24 from IP address 90.246.25.176. Copyright ARRS. For personal use only; all rights reserved AJR:194, June 2010 1677 MRI-Occult Breast Cancers median size of the false-negative lesions on final pathology evaluation was 10 mm. There were four false-negative DCIS lesions, one of which was very small by pa[1]thology (5 mm) (Fig. 1). Two other DCIS lesions were obscured by diffusely enhancing surrounding parenchyma (Fig. 2) even at the early phase (75 seconds) of the dynamic study. The remaining multifocal DCIS lesion (grade 3) did not show enhancement in a background of minimal parenchymal enhancement for reasons that are not known. There were three false-negative invasive carcinomas. One 8-mm IDC with extensive DCIS was obscured by diffusely enhancing surround[1]ing parenchyma (Fig. 3). One very small (0.8 mm) IDC with DCIS did not show enhancement in a background of mild parenchymal enhancement for reasons that are not known. The remaining lesion, IDC with DCIS, was visible on T2-weighted images as a low-signal mass; however, no enhancement was noted after the administration of contrast medium. Discussion In this study, DCE-MRI offered a high sensitivity in a cohort of patients with newly diagnosed breast cancer. Sensitivity for all breast carcinoma, invasive carcinoma, and in situ carcinoma was 96.8%, 98.3%, and 90.2%, respec[1]tively. These results are comparable or slightly superior to previously published results [18– 20] (Table 3). This improvement could be explained by the more modern technical parameters used compared with those of prior studies—that is, higher field strength (1.5 T), higher temporal resolution (75 seconds), and higher spatial resolution (slice thickness, 2 mm; in-plane resolution, 1–1.5 mm). The percentage of palpable lesions in this study (84/164 lesions, 51%), when known, was similar to or lower than the percentage of palpable findings in previously reported studies [7, 20]. However, there are some differences in study methodology when this experience is compared with prior reports [18, 20]. Entry criteria in these prior studies include patients with histologically proven benign lesions and those with malignant lesions. In contrast, the reported sensitivity in this study and in the study by Ghaiet al. [19], both retrospective studies, was achieved in cases in which readers knew malignancy was present before reading MRI studies. In the study by Schnall et al. [20], 13 (3.1%) of 422 invasive lesions and 12 (15.6%) of 77 DCIS lesions did not exhibit enhancement at MRI. Teifke et al. [18] found that 28 (8.4%) of 334 invasive lesions and 13 (65%) of 20 DCIS lesions were missed at MRI. In addition, unlike the cases presented in this report, the false-negative lesions described by Teifke et al. included malignancies that were not detected because of technical reasons. No technically inadequate examinations compromised this study and none were included in that of Ghai et al. Despite these differences in study design, the results of this study and all other studies show the existence of MRI-occult breast malignancies. In this study, seven cancers (3.2%) showed no enhancement on MRI. Of the seven false[1]negative cases, four malignancies represented pure DCIS. Pure DCIS lesions often present as nonmass, clumped enhancement in a segmental or linear distribution [23] with plateau or washout curve types [22–25] but with lower peak enhancement values. Non-mass-like enhancement may be more difficult to perceive TABLE 3: Data From Published Articles Compared With Data From This Study Journal, Year of Publication First Author [Reference No.] Total No. of Lesions No. of False-Negative Lesions Sensitivity (%) Total Invasive Cancer In Situ Cancer Total Invasive Cancer In Situ Cancer AJR, 2005 Ghai [19] 104 9 9 — 91.3 91.3 — Radiology, 2002 Teifke [18] 354 41 28 13 88.4 91.6 35.0 Radiology, 2006 Schnall [20] 995 25 13 12 95.0 96.9 84.4 This study 220 7 4 3 96.8 98.3 90.2 Note—Dash (—) indicates no ductal carcinoma in situ present in this population. A Fig. 2—43-year-old woman with screening-detected pleomorphic calcifications measuring 2.5 cm in right breast (case 2 in Table 2). Stereotactic core biopsy revealed ductal carcinoma in situ (DCIS), grade 3. A, Craniocaudal mammographic view of right breast obtained after stereotactic core biopsy shows residual calcifications (arrows). B, On early phase of dynamic contrast-enhanced study (subtraction, T1-weighted images), no abnormal enhancement is observed at area of susceptibility artifact from metallic clip placed after stereotactic core biopsy (arrow) because of diffuse parenchymal enhancement. Needle localization lumpectomy revealed DCIS, grade 3, measuring 3 cm. B Downloaded from ajronline.org by 90.246.25.176 on 02/27/24 from IP address 90.246.25.176. Copyright ARRS. For personal use only; all rights reserved 1678 AJR:194, June 2010 Shimauchi et al. especially in the presence of enhancing breast parenchyma. This observation is supported by a report from the MRI Lexicon Committee indicating that reader agreement for the classification of linear enhancement distribution was poor [24]. There were three cases (two DCIS and one IDC with DCIS) in patients who were younger than the median age of the patient cohort with diffusely enhancing surrounding parenchyma, that could obscure an abnormal enhancing lesion. The median age of these three patients was 46 years, whereas the median age of newly diagnosed cancer patients overall was 58 years. One limitation of this study is that we did not take the hormonal status of our patients into account for scheduling the examinations. At our institution, scheduling patients for breast MRI to stage newly diagnosed cancer has not routinely been done according to the phase in the menstrual cycle for premenopausal women. Perhaps imaging in the second week or at least in the middle of the menstrual cycle, as advocated by Viehweg et al. [26] and Müller-Schimpfle et al. [27], might reduce the number of cases with false-negative MRI due to diffusely enhancing surrounding parenchyma. However, this type of scheduling can be psychologically stressful for patients and can present a perceived delay in care. Of the remaining false-negative malignancies, one was a small (0.8 mm) IDC with DCIS. Teifke et al. [18] suggested that infiltrating cancers associated with DCIS might be difficult to detect on MRI. The sensitivity of MRI for DCIS reported by Teifke et al. was 35%, and those investigators concluded that MRI cannot reliably diagnose DCIS-positive cancers. Although there are some differences in the study methodologies in this study, the sensitivity for DCIS was 90.2%, which suggests that improvement in DCE-MRI technique may aid in achieving a higher sensitivity for DCIS. Further studies are required to prove a definitive association between false-negative MRI examinations and DCIS lesions. Other invasive cancers may not be visualized readily because of very small size or because of diffuse pattern of spread. Prior studies have shown ILC to be MRI occult because of diffuse infiltration without mass formation [16, 17, 19]. However, in this study, all ILC lesions (8.6% of total malignancies) were detected at MRI. The relatively thicker slice thickness (range, 3–10 mm) used in pri[1]or reported studies could have negatively impacted the sensitivity of MRI for ILC. A limitation of this study includes a possible bias because it is a retrospective review. At the time of the retrospective read for this study, re[1]viewers were aware of both the initial and the final histologic findings. In routine practice, we may not be aware of all of the details concerning the histology for all cases, although we routinely have histology or cytology findings for most staging MRI cases at the time of the prospective read. However, this study has shown that improved technical parameters— that is, a higher field strength (1.5 T), higher temporal resolution, higher spatial resolution, and improved coil design—led to better results for the detection of small malignant lesions, particularly DCIS. To summarize, in a population of 220 sequentially diagnosed known breast cancer lesions, we found seven (3.2%) MRI-occult cancers, which is fewer than reported in other published studies. Small tumor size and dif[1]fuse parenchymal enhancement were likely the principal reasons for these false-negative results. Although the overall sensitivity of breast MRI for cancer detection was high (96.8%), it should be emphasized that a negative MRI should not influence the management of a lesion that appears to be of concern on physical examination, mammography, or ultra[1]sound. MRI is complementary to—but is not a replacement for—other breast imaging techniques and should not be used as the sole imag[1]ing study because, as this study shows, a small number of cancers may not be visible at MRI. References 1. Harms SE, Flamig DP, Hesley KL, et al. MR imaging of the breast with rotating delivery of excitation off resonance: clinical experience with pathologic correlation. Radiology 1993; 187:493–501 2. Gilles R, Guinebretiere JM, Lucidarme O, et al. Nonpalpable breast tumors: diagnosis with contrast-enhanced subtraction dynamic MR imaging. Radiology 1994; 191:625–631 3. Kaiser WA. False-positive results in dynamic MR A Fig. 3—49-year-old woman with diffuse pleomorphic and linear calcifications measuring 6.5 cm in right breast, proven to be DCIS, grade 2, by stereotactic core biopsy (case 6 in Table 2). A, Mediolateral magnification view of right breast obtained after stereotactic core biopsy shows calcifications (arrows). Metallic clip (arrowhead) was placed in upper inner quadrant. B, On early phase of dynamic contrast-enhanced study (subtraction, T1-weighted images), no abnormal enhancement is observed in upper outer quadrant of right breast because of diffuse parenchymal enhancement. Right simple mastectomy revealed 8-mm invasive ductal carcinoma, grade 2, with extensive ductal carcinoma in situ. B Downloaded from ajronline.org by 90.246.25.176 on 02/27/24 from IP address 90.246.25.176. Copyright ARRS. For personal use only; all rights reserved AJR:194, June 2010 1679 MRI-Occult Breast Cancers mammography: causes, frequency, and methods to avoid. Magn Reson Imaging Clin N Am 1994; 2:539–555 4. Fobben ES, Rubin CZ, Kalisher L, Dembner AG, Selt[1]zer MH, Santoro EJ. Breast MR imaging with commercially available techniques: radiologic–pathologic correlation. Radiology 1995; 196:143–152 5. Bone B, Aspelin P, Bronge L, Isberg B, Perbeck L, Veress B. Sensitivity and specificity of MR mam[1]mography with histopathological correlation in 250 breasts. Acta Radiol 1996; 37:208–213 6. Liberman L, Morris EA, Dershaw DD, Abramson AF, Tan LK. MR imaging of the ipsilateral breast in women with percutaneously proven breast can[1]cer. AJR 2003; 180:901–910 7. Berg WA, Gutierrez L, NessAiver MS, et al. Diag[1]nostic accuracy of mammography, clinical exami[1]nation, US, and MR imaging in preoperative as[1]sessment of breast cancer. Radiology 2004; 233:830–849 8. Sardanelli F, Giuseppetti GM, Panizza P, et al. Sensitivity of MRI versus mammography for detecting foci of multifocal, multicentric breast cancer in fatty and dense breasts using the whole[1]breast pathologic examination as a gold standard. AJR 2004; 183:1149–1157 9. Schnall MD, Blume J, Bluemke DA, et al. MRI detection of distinct incidental cancer in women with primary breast cancer studied in IBMC 6883. J Surg Oncol 2005; 92:32–38 10. Hollingsworth AB, Stough RG. Preoperative breast MRI for locoregional staging. J Okla State Med Assoc 2006; 99:505–515 11. Bilimoria KY, Cambic A, Hansen NM, Bethke KP. Evaluating the impact of preoperative breast magnetic resonance imaging on the surgical management of newly diagnosed breast cancers. Arch Surg 2007; 142:441–445; discussion, 445–447 12. Lehman CD, Gatsonis C, Kuhl CK, et al. MRI evaluation of the contralateral breast in women with recently diagnosed breast cancer. N Engl J Med 2007; 356:1295–1303 13. Van Goethem M, Schelfout K, Kersschot E, et al. MR mammography is useful in the preoperative locoregional staging of breast carcinomas with extensive intraductal component. Eur J Radiol 2007; 62:273–282 14. Braun M, Polcher M, Schrading S, et al. Influence of preoperative MRI on the surgical management of patients with operable breast cancer. Breast Cancer Res Treat 2008; 111:179–187 15. Kaiser WA. MR mammography [in German]. Ra[1]diologe 1993; 33:292–299 16. Boetes C, Strijk SP, Holland R, Barentsz JO, Van Der Sluis RF, Ruijs JH. False-negative MR imag[1]ing of malignant breast tumors. Eur Radiol 1997; 7:1231–1234 17. Wurdinger S, Kamprath S, Eschrich D, Schneider A, Kaiser WA. False-negative findings of malig[1]nant breast lesions on preoperative magnetic reso[1]nance mammography. Breast 2001; 10:131–139 18. Teifke A, Hlawatsch A, Beier T, et al. Undetected malignancies of the breast: dynamic contrast-en[1]hanced MR imaging at 1.0 T. Radiology 2002; 224:881–888 19. Ghai S, Muradali D, Bukhanov K, Kulkarni S. Nonenhancing breast malignancies on MRI: sonographic and pathologic correlation. AJR 2005; 185:481–487 20. Schnall MD, Blume J, Bluemke DA, et al. Diag[1]nostic architectural and dynamic features at breast MR imaging: multicenter study. Radiology 2006; 238:42–53 21. Van Goethem M, Schelfout K, Kersschot E, et al. Comparison of MRI features of different grades of DCIS and invasive carcinoma of the breast. JBR-BTR 2005; 88:225–232 22. Jansen SA, Newstead GM, Abe H, Shimauchi A, Schmidt RA, Karczmar GS. Pure ductal carcino[1]ma in situ: kinetic and morphologic MR charac[1]teristics compared with mammographic appear[1]ance and nuclear grade. Radiology 2007; 245:684–691 23. Shiraishi A, Kurosaki Y, Maehara T, Suzuki M, Kurosumi M. Extension of ductal carcinoma in situ: histopathological association with MR imag[1]ing and mammography. Magn Reson Med Sci 2003; 2:159–163 24. Ikeda DM, Hylton NM, Kinkel K, et al. Develop[1]ment, standardization, and testing of a lexicon for reporting contrast-enhanced breast magnetic res[1]onance imaging studies. J Magn Reson Imaging 2001; 13:889–895 25. Menell JH, Morris EA, Dershaw DD, Abramson AF, Brogi E, Liberman L. Determination of the presence and extent of pure ductal carcinoma in situ by mammography and magnetic resonance imaging. Breast J 2005; 11:382–390 26. Viehweg P, Paprosch I, Strassinopoulou M, Hey[1]wang-Köbrunner SH. Contrast-enhanced magnetic resonance imaging of the breast: interpreta[1]tion guidelines. Top Magn Reson Imaging 1998; 9:17–43 27. Müller-Schimpfle M, Ohmenhaüser K, Stoll P, Dietz K, Claussen CD. Menstrual cycle and age: influence on parenchymal contrast medium enhancement in MR imaging of the breast. Radiology 1997; 203:145–
Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA Woo-Suk Chung, M.D.1 , Tae-Sub Chung, M.D.1 , Hyung Jung Kim, M.D.2 , Chul Min Ahn, M.D.2 , Jae Hoon Lee, M.D.1 , Jin Hur, M.D.1 , Arthur Eung-Hyuck Cho, M.D.1 Purpose : Early detection of small brain metastases is important. The purpose of this study was to compare the detectability of brain metastases according to the size between 1.5 T and 3.0 T MRI. Materials and Methods : We reviewed 162 patients with primary lung cancer who were examined for TNM staging. After administration of double dose of Gd-DTPA, MR imaging was performed with SPGR by 3.0 T MRI and then with T1 SE sequence by 1.5 T MRI. In each patient, three readers performed qualitative assessment. Sensitivity, positive predictive value, and diagnostic accuracy were calculated in 3.0 T and 1.5 T MRI according to size. Using the signal intensity (SI) measurements between the metastatic nodules and adjacent tissue, nodule-to-adjacent tissue SI ratio was calculated. Results : Thirty-one of 162 patients had apparent metastatic nodules in the brain at either 1.5 T or 3.0 T MR imaging. 143 nodules were detected in 3.0 T MRI, whereas 137 nodules were detected at 1.5 T MRI. Six nodules, only detected in 3.0 T MRI, were smaller than 3.0 mm in dimension. Sensitivity, positive predictive value, and diagnostic accuracy in 3.0 T MRI were 100 %, 100 %, and 100 % respectively, and in 1.5 T MRI were 95.8 %, 88.3 %, and 85.1 % respectively. SI ratio was significantly higher in the 3.0 T MRI than 1.5 T MRI (p=0.025). Conclusion : True positive rate of 3.0 T MRI with Gd-DTPA was superior to 1.5 T MRI with Gd-DTPA in detection of metastatic nodules smaller than 3.0 mm. Index words :Magnetic resonance (MR), high-field-strength imaging Brain neoplasm, metastases Contrast medium Introduction Brain metastases present a poor prognosis suggesting a shortened survival time. Early diagnosis of brain involvement and determination of the number of metastases are important not only for quality of life but also for cost effectiveness (1-3). The decision regarding a conservative versus a surgical approach depends on the number of brain metastases detected by radiologic means (1-3). A contrast-enhanced MRI has become the method of choice for visualization of brain metastases (1). Highdose gadolinium-enhanced MR examinations may have advantages over 0.1 mmol/kg examinations in detecting early and/or small metastases (3-7). A delayed study can also increase the contrast (2). Comparing to the 1.5 T MRI with an axial T1-weighted spin echo sequence (SE), the higher field strength MR systems combined with a sequence of SPGR (spoiled gradient recalled acquisition in the steady state) and administration of a high dose of Gd-DTPA (gadopentetate dimeglumine) may also have advantages in detecting small metastases, although this has not yet been verified by clinical data. The purpose of this study is to compare the detectability of brain metastases classified according to the size of nodules, between thin slice SPGR of 3.0 T and conventional thick slice SE of 1.5 T MRI with the administration of a double dose of GdDTPA. Materials and Methods Patients From December 2002 to February 2004, a total of 162 consecutive patients with primary lung cancer participated in our study. The institutional review board approved our study, and informed consent was obtained from all patients regarding the potential risks of both the double dose of contrast medium and two assessments by MRI scanning on a 3.0 T and 1.5 T machine. After the study, 31 patients of this population were diagnosed as having brain metastases. Mean patient age was 61.2 (range, 43 to 80 years). Protocol On the 3.0 T MR scanner (GE Signa VH/i; GE medical system, Milwaukee, USA), the images were acquired using a standard head coil and an actively shielded gradient system with a maximum gradient strength of 43 mT/m. On the 1.5 T MR scanner (Magnetom Vision; Siemens Medical Systems, Erlangen, Germany), a standard head coil and a maximum gradient strength of 25 mT/m were used. All patients were examined after administrating a contrast agent with a double dose of Gd-DTPA (0.2 mmol/kg). First, examinations were performed on a 3.0 T MR scanner and then were subsequently performed on a 1.5 T MR scanner without additional contrast injection. The scan interval between the 3.0 T and 1.5 T MR examination was less than 20 minutes. The contrast agent used was Gd-DTPA (Magnevist; Schering AG, Berlin, Germany). In all patients, the double dose of Gd-DTPA at 0.2 mmol/kg was administered intravenously as a bolus and scanning commenced immediately. MR imaging included the following sequences on both scanners: At 3.0 T MRI, an axial 3D SPGR, which is usually used at present, was used (TR/TE/TI = 5.7/1.44/400 milliseconds; flip angle 20°; 2 mm slice thickness; FOV of 220 mm; matrix size of 512×512 ZIP; spatial resolution of 0.43×0.43×2 mm; two acquisition) with a scan time of 3 minutes 30 seconds. At 1.5 T MRI, an axial T1-weighted spin echo sequence was used (TR/RE = 600/14 milliseconds; flip angle 90°; 5 mm slice thickness; FOV of 210 mm; matrix size of 174×256; spatial resolution of 1.2×0.82×5 mm; two acquisition) with a scan time of 5 minutes 30 seconds. Three radiologists performed randomized, independent blinded review. The three readers were merely informed that all of the patients had lung malignancies. The postcontrast MR examinations of the brain on all of the patients were evaluated. The readers did not have access to other image sets within each study. The presence, size, and number of metastatic nodules were assessed. The postcontrast images were divided into the following two groups: 3.0 T MRI with a double dose of Gd-DTPA and 1.5 T MRI with a double dose of Gd-DTPA. The readers were asked to document the number of nodules. Each nodule in each study was numbered and classified according to its largest diameter measurement: ≤3 mm, 3 mm to 5 mm, or 5 mm. Woo-Suk Chung et al
102 – Subsequently, if there was any debate about nodule classification, a final interpretation using imaging studies was done until consensus among the readers was accomplished. If disagreements persisted, 3-6 months of follow-up MR scans were obtained for further validation. For the patients who had follow-up MR scans, these scans were considered positive for metastases if there was a response to the treatment or if there was a growth of nodules identified during the follow-up period. In addition, the sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of the 3.0 T and 1.5 T MRI were calculated using the results from the final interpretation according to size. A quantitative image assessment was performed next. The same lesions on scans of the two different MRI systems were determined by comparing peripheral structures. Signal intensities of adjacent tissue and nodule were assessed by region of interest (ROI) measurements placed identically on both series of images using the same sized circular ROI from the software available on both scanners. Nodule-toadjacent tissue contrast (SI ratio) is defined by SI ratio = ×100 Stissue1 taken as the signal intensity of an ROI assessed over a nodule and Stissue2 taken as the signal intensity assessed over the contralateral white matter. The signal intensity of a nodule was measured within an enhanced area. In inhomogeneously enhanced nodules, the area of maximum uptake was chosen for measurement. Statistical Analysis The paired Wilcoxon’s signed ranks test was used to compare qualitative scores, and the matched-pair-t test was used to compare nodule SI ratios between the 3.0 T and 1.5 T MRI with a double dose of Gd-DTPA. For all tests, significance was set at p < 0.05, and SPSS software (SPSS Inc. Chicago, US) was used for statistical analyses. Results In the final review made by consensus of three radiologists (Table 1), a total of 143 metastatic nodules were detected by the 3.0 T MRI with a double dose of Gd-DTPA. Of these nodules, 49 nodules were ≤ 3 mm in diameter, 37 nodules were 3 mm to 5 mm, and 57 nodules were >5 mm. A total of 137 metastatic nodules were detected by the 1.5 T MRI with a double dose of Gd-DTPA in the final interpretation. Of these nodules, 43 nodules were ≤ 3 mm in diameter. The 3.0 T MRI with a double dose of Gd-DTPA was significantly more effective at detecting nodules smaller than 3 mm (p = 0.014) than the 1.5 T MRI. However, we found no significant difference in the detection of nodules larger than 3 mm (p > 0.05) (Table 1). In 6 of the 31 cases, six nodules, which were only detected by the 3.0 T MRI with a double dose of GdDTPA, and missed by the 1.5 T MRI with a double dose of Gd-DTPA, were unanimously agreed upon by all participants in the final interpretation. In three of the six nodules, a growing nodule was detected during a follow-up MR scan which confirmed the presence of metastases (Fig. 1). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of Gd-DTPA due to artifact (Fig. 2). Finally the 3.0 T MRI with a double dose of Gd-DTPA was Stissue1 – Stissue2 Stissue2 Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA
103 – Table 1. Total Number of Brain Metastases Classified by Size and Detected at the Final Interpretation Size 3.0 T MRI with 1.5 T MRI with p value Gd-DTPA Gd-DPTA ≤ 3 mm 49 43 0.014 3 mm<-≤5 mm 37 37 > 0.05 5 mm< 57 57 > 0.05 Total 143 137 0.014 Note : Data are the number of nodules Table 2. The Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRIs with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm Present Absent Present Absent 3.0 T MRI with Positive 143 00* 49 0* Gd-DTPA Negatiive 000 00* 00 0* 1.5 T MRI with Positive 137 18* 43 18* Gd-DTPA Negative 006 00* 06 0*
Pseudolesions that were detected as nodules by the 1.5 T MRI were detected as vascular structures by the 3.0 T MRI. useful for confirming the presence of these nodules. Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter or better delineation than by the 1.5 T MRI with a double dose of Gd-DTPA. Out of 137 nodules, 65 were brighter (Fig. 3) and out of 137 nodules, 63 were better delineated (Fig. 4). Fortyfive of 137 nodules were satisfactory in both conditions. By consensus, the final review stated, nodules detected by the 3.0 T and 1.5 T MRI were considered positive for metastases (Table 2). Additionally, there were 18 pseudolesions which were detected as nodules by the 1.5 T MRI, but as vascular structures by the 3.0 T MRI (Fig. 5). The sensitivity, positive predictive values, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 95.8%, 88.3%, and 85.1% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of the 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and Woo-Suk Chung et al
104 – a b Fig. 2. A 73-year-old male with multiple brain metastases. Metastatic nodule (a) by a 3.0 T MR image with a double dose of Gd-DTPA show a metastatic nodule (arrow). But (b) the 1.5 T MR image with a double dose of Gd-DTPA cannot show the metastatic nodule by artifact. abc Fig. 1. A 65-year-old male with single brain metastasis. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a small metastatic nodule (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA cannot show the nodule. In (c), a growing nodule was detected during the follow-up MRI with a double dose of Gd-DTPA which confirmed the presence of metastasis (arrow). 100% respectively. For metastatic nodules smaller than 3 mm, the sensitivity, positive predictive value, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 87.8%, 70.5%, and 64.2% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and 100% respectively (Table 3). For quantitative image assessment, the SI ratio in the post contrast sequences (Table 4) was significantly higher in the 3.0 T MRI with a double dose of GdDTPA than in the 1.5 T MRI with a double dose of GdDTPA (p = 0.025). Discussion Detection of metastatic nodules is dependent on both their size and contrast ratio (2). As methods to increase the contrast, a higher dose of Gd-DTPA, a higher field strength, and delayed study can all be used to aid detection (2-5, 8-17). Nodules larger than 10 mm are easily detected because vasogenic edema is customarily associated with larger metastases (2). So, when a higher dose of Gd-DTPA is used, the detection rate of larger nodules is not influenced. However, a higher dose is helpful for detecting small nodules because it increases nodule enhancement, yet this method has the disadvantages of increasing the false positive rate and promoting side effects (2-5, 8-14). A delayed study can also increase the contrast (2). It has been recommended that image acquisition be delayed from 5 to 35 minutes after the administration of contrast material at a dose of 0.1 mmol/kg to ensure optimal detection (2, 15). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of GdDTPA due to partial volume artifact. Eighteen lesions were detected in the 1.5 T MRI with a double dose of Gd-DTPA, which proved to be vascular structures in 3.0 T MRI with a double dose of Gd- DTPA. The true nature of these lesions was revealed because of the greater morphologic detail visualized by the high field Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA
105 – a b Fig. 3. A 65-year-old male with multiple brain metastases. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhancement (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhancement (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter than when observed by the 1.5 T MRI with a double dose of GdDTPA. Table 3. Estimation of the Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRI with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm 3.0 T 1.5T 3.0 T 1.5T Sensitivity 100 95.8 100 87.8 Specificity – 0 – 0 Positive predictive value 100 88.3 100 70.5 Negative predictive value – 0 – 0 Diagnostic accuracy 100 85.1 100 64.2 Table 4. Results of a quantitative assessment of nodules that were detected by the 3.0 T and 1.5 T MRIs with Gd-DTPA (n=137) 3.0 T 1.5 T P value Nodules-to-adjacent tissue: SI ratio 94.59 63.86 0.025 strength MR image, thus allowing differentiation between true enhancing lesions and sulcal vessels. In our study, each nodules was classified according to its largest diameter as being ≤ 3 mm, 3 mm to 5 mm, and >5 mm because the slice thickness of the 3.0 T MRI was 2.0 mm and 5 mm for the 1.5 T MRI. Therefore this study classified small metastatic nodules as being smaller than 3 mm. Although our study supports the use of a higher field strength MRI with a double dose of Gd-DTPA for increased metastatic nodule detection and for improved nodule enhancement and delineation, the results should be interpretated with caution. The reason for this is that for patients with two or more brain metastases, additional metastases found with the 3.0 T MRI seem to be of limited clinical importance. The presence of two or more small nodules generally will not change the way the patient is managed. Therefore, it is of utmost importance to identify the difference between none, one, and more than one metastatic nodule. Patients with a single metastatic nodule located in a respectable region can be treated surgically, and the tumor staged as M1, not M0. However, patients with two or more metastatic nodules are usually Woo-Suk Chung et al
106 – a b Fig. 5. A 67-year-old female with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows vascular structure (arrow). (b) The 1.5 T MRI with a double dose of GdDTPA shows a nodular lesion (arrow). A pseudolesion that was detected as a nodule by the 1.5 T MRI with a double dose of GdDTPA but as a vascular structure by the 3.0 T MRI with a double dose of Gd-DTPA is showed in this figure. a b Fig. 4. A 64-year-old male with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows a metastatic nodule with ring enhancement (arrow). (b) The 1.5 T MRI with Gd-DTPA show a metastatic nodule with ring enhancement (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were better delineated than when observed by the 1.5 T MRI with a double dose of GdDTPA. treated with radiation therapy and/or systemic chemotherapy (3, 18-22). On the other hand, the use of a higher strength field MRI was found to be helpful in confirming the appearance of an equivocal metastatic nodule. The 3.0 T MRI with a double dose of Gd-DTPA was also useful for the detection of additional metastases in patients with a known lesion detected by the 1.5 T MRI with a double dose of GdDTPA. Because this also has influence on the sensitivity, positive predictive value, and diagnostic accuracy the 3.0 T MRI with a double dose of GdDTPA was found to have better results than the 1.5 T MRI with a double dose of Gd-DTPA in our study. Therefore we recommend the use of the 3.0 T MRI with a double dose of Gd-DTPA in only three circumstances: when the findings by the 1.5 T MRI with Gd-DTPA are equivocal, when one potentially surgically respectable nodule is identified, or for detecting early and/or small metastases There were two limitations in this study. The first limitation was a difference in protocol sequence. The T1 weighted spin-echo protocol was used for the 1.5 T MRI and SPGR technique protocol for the 3.0 T MRI. Detectability of metastatic nodules is more effective with 3.0 T MRI with T1 SE than with a 1.5 T MRI with SE (2). SPGR with thin slice thickness is superior to the T1 spin echo sequence with thick slice thickness due to a partial volume effect. Additionally, SE is not optimum for a 3.0 T due to longer T1- and shorter T2- relaxation times of water protons, which decrease the contrast ratio in the 3.0 T images.17 The purpose of this study was to detect early small brain metastases, so using the SPGR sequence with a 3.0 T MRI, which is usually used at present, has advantages for detecting early small brain metastases. The second limitation was that the scan interval between the 1.5 T and 3.0 T MRI was less than 20 minutes. However, a delayed study increases contrast as mentioned above. The current study found that the SI ratio was significantly higher in the 3.0T images than in the 1.5 T images. Considering the delayed study by the 1.5 T MRI, this limitation emphasizes the better detection rate of the 3.0 T MRI with a double dose of Gd-DTPA. And due to these confounding variables, blinded reviews were performed by three readers. The detectability of metastatic nodules smaller than 3mm was better using a 3.0 T MRI with SPGR than a 1.5 T MRI with T1 SE. Therefore we recommend a 3.0 T MRI with SPGR and a double dose of Gd-DTPA for detecting early and/or small metastatic nodules, furthermore influencing treatment. References 1.Lassman AB, DeAngelis LM. Brain metastases. Neurol Clin. 2003; 21:1-23, vii, Review 2.Ba-Ssalamah A, Nobauer-Huhmann IM, Pinker K, et al. Effect of contrast dose and field strength in the magnetic resonance detection of brain metastases. Invest Radiol 2003; 38: 415-422 3.Sze G, Johnson C, Kawamura Y, et al. Comparison of singleand triple-dose contrast material in the MR screening of brain metastases. AJNR Am J Neuroradiol 1998; 19:821-828 4.Runge VM, Kirsch JE, Burke VJ, et al. High-dose Gadoteridol in MR imaging of intracranial neoplasm. J Magn Reson Imaging 1992; 2:9-18 5.Yuh WT, Engelken JD, Muhonen MG, Mayr NA, Fisher DJ, Ehrhardt JC. Experience with high-dose gadolinium MR imaging in the evaluation of brain metastases. AJNR Am J Neuroradiol 1992; 13:335-345 6.Brekenfeld C, Foert E, Hundt W, Kenn W, Lodeann KP, Gehl HB. Enhancement of cerebral diseases: How much contrast agent is enough? Comparison of 0.1, 0.2, and 0.3 mmol/kg Gadoteridol at 0.2 T with 0.1 mmol/kg Gadoteridol at 1.5 T. Invest Radiol 2001; 36:266-275 7.Yuh WT, Tali ET, Nguyen HD, Simonson TM, Mayr NA, Fisher DJ. The effect of contrast dose, imaging time, and lesion size in the MR detection of intracerebral metastasis. AJNR Am J Neuroradiol 1998; 16:373-380 8.Van Dijk P, Sijens PE, Schmitz PI, Oudkerk M. Gd-enhanced MR imaging of brain metastases: contrast as a function of dose and lesion size. Magn Reson Imaging 1997; 15:535-541 9.Yuh WT, Fisher DJ, Engelken JD, et al. MR evaluation of CNS tumors: dose comparison study with gadopentetate dimeglumine and gadoteridol. Radiology 1991; 180:485-491 10.Healy ME, Hasselink JR, Press GA, Middleton MS. Increased detection of intracranial metastases with intravenous GdDTPA. Radiology 1987; 165:619-624 11.Akeson P, Vikhoff B, Stahlberg F, Holtas S. Brain lesion contrast in MR imaging: dependence of field strength and concentration of gadodiamide injection in patients and phantoms. Acta Radiol 1977; 38:14-18 12.Runge VM. A review of contrast media research in 1999 –
Invest Radiol 2001; 36:123-130 13.Yuh WT, Parker JR Carvlin MJ. Indication related dosing for magnetic resonance contrast media. Eur Radiol 1977; 7(suppl 5):S269-S275 14.Rinck PA, Muller RN. Field strength and dose dependence of contrast enhancement by Gadolinium-based MR contrast agents. Eur Radiol 1999; 9:998-1004 15.Schorner W, Laniado M, Niendorf HP, Schubert C, Felix R. Time-dependent changes in image contrast in brain tumors after gadolinium-DTPA. AJNR Am J Neuroradiol 1986; Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA
107 – 7:1013-1020 16.Chang KH, Ra DG, Han MH, Cha SH, Kim HD, Han MC. Contrast enhancement of brain tumors at different MR field strengths: comparison of 0.5 T and 2.0 T. AJNR Am J Neuroradiol 1994; 15:1413-1419 17.Nobauer-Huhmann IM, Ba-Ssalamah A, Mlynarik V, et al. Magnetic resonance imaging contrast enhancement of brain tumors at 3 tesla versus 1.5 tesla. Invest Radiol 2002; 37:114- 119 18.Galicich JH, Sundaresan N, Thaler HT. Surgical treatment of single brain metastasis: evaluation of results by computerized tomography scanning. J Neurosurg 1980; 53:63-67 19.Runge VM, Carollo BR, Wolf CR, Nelson KL, Gelblum DY. Gd-DTPA: A review of clinical indications in central nervous system magnetic resonance imaging. Radiographics 1989; 9:929-958 20.Earnest F 4th, Ryu JH, Miller GM, et al. Suspected non-small cell lung cancer: Incidence of occult brain and skeletal metastases and effectiveness of imaging for detection-Pilot study. Radiology 1999; 211:137-145 21.Koutras AK, Marangos M, Kourelis T, et al. Surgical management of cerebral metastases from non-small cell lung cancer. Tumori 2003; 89:292-297 22.Soffietti R, Ruda R, Mutani R. Management of brain metastases. J Neurol 2002; 249:1357-1369. Review Woo-Suk Chung et al
108 – 통신저자 : 정태섭, 서울특별시 강남구 도곡동 146-92 연세대학교 영동세브란스병원 영상의학과 Tel. 82-2019-3514 Fax. 82-3462-5472 E-mail: tschung@yumc.yonsei.ac.kr 뇌전이종양의발견에있어서Doble dose Gd-DTPA를이용한 3 T MRI와1.5 T MRI간의비교연구 1 연세대학교 영동세브란스병원 영상의학과 2 연세대학교 영동세브란스병원 호흡기내과 정우석1 ·정태섭1 ·김형중2 ·안철민2 ·이재훈1 ·허 진1 ·조응혁1 목적: 작은 뇌전이 종양의 조기 발견은 중요하다. 이 연구의 목적은 1.5 T MRI와 3.0 T MRI 간의 크기에 따른 뇌 전이 종양의 발견율을 비교하는 것이다. 대상 및 방법: 폐암으로 진단 받은 162명의 환자를 대상으로 TNM 병기를 위해 뇌 MRI를 시행하였다. Gd-DTPA 를 2배 용량으로 투여 후, 3.0 T MRI에서 훼손경사회복획득으로 촬영하였으며 그 후 1.5 T MRI에서 T1 스핀 에 코로 촬영하였다. 3명의 방사선과 전문의가 합의하여 MRI를 판독하였으며 정성 평가를 시행하였다. 3.0 T와 1.5 T MRI에서 크기에 따라 민감도, 양성 예측률, 정확도를 평가하였다. 신호 강도를 사용하여 전이 종양과 인접 조직간 의 신호강도 비를 계산하였다. 결과: 162명의 환자 중 31명에서 1.5 T 또는 3.0 T MR에 뇌전이 종양이 발견되었다. 3.0 T MRI에서 143개의 종 양이 발견되었으나 1.5 T MRI에서 137개의 종양이 발견되었다. 6개의 종양이 3.0 T MRI에서만 발견되었으며 크 기는 모두 3 mm 미만이었다. 3.0 T MRI의 민감도, 양성 예측률, 정확도는 각각 100%, 100%, 100%이며, 1.5 T MRI에서는 각각 95.8%, 88.3%, 85.1% 이다. SI ratio는 1.5 T MRI보다 3.0 T MRI에서 유의하게 높았다 (p=0.025). 결론: Double dose Gd-DTPA를 이용한 3.0 T MRI는 3 mm미만의 뇌전이 종양을 발견하는데 있어서 1.5 T MRI 보다 우수하다.
4/16/20
Malcolm’s brain MRI was initially read as completely normal. Upon getting a second opinion, it was discovered that 22 lesions suggestive of multiple sclerosis had been missed. Here is his story.
[Malcolm] After 18 months of deteriorating health, with a multitude of neurological symptoms, I went to see a neurologist. I was ordered a standard brain MRI to help figure out what was going on. By this time, I had been researching my symptoms for a few months, and, in doing so, had developed a basic understanding of what I was looking for: T2 lesions.
When I received the results from my MRI, the report said everything was normal. I met with my neurologist, and he too said there was nothing abnormal about my scan. When I viewed the MRI myself, however, I found 4 spots that looked to me to be brain lesions. I brought them up to my doctor at my next appointment but was essentially laughed at.
It was quite unsettling to have something so concerning be shrugged off. After that appointment, I decided I wanted to switch to a new neurologist and get a second opinion on my MRI scan. I made an appointment with the new doctor, but it was going to be another 6 weeks before I could be seen. Fortunately, I found DocPanel. I submitted my MRI for review and, within 48 hours, I got my results back.
[Dr. Michael Rozenfeld] Malcolm reached out to DocPanel due to concern for a missed diagnosis. He was reportedly having symptoms suspicious for multiple sclerosis but his MRI was initially read as completely normal. Based on my review of his MRI, the exam was not normal. Malcolm had significant findings that were certainly suggestive of, but not entirely specific for, multiple sclerosis.
[Malcolm] My second opinion results were quite alarming – there were not 4 lesions, but 22. Twenty-two! They were small, but they were most definitely there. I took the second opinion report to my new neurologist, and now I am being considered for possible Primary Progressive Multiple Sclerosis. I am scheduled to get new MRIs in November to confirm or rule out MS and you can be sure I will be sending them to DocPanel for a second look!
I have found that the most important thing people in my shoes can do is be your own advocate. MS is such an odd and individual disease. – Malcolm
[Dr. Michael Rozenfeld] Radiology exams can be misinterpreted for a number of reasons – this is unfortunately not uncommon. While MRI is not the only piece in the puzzle for MS diagnosis, it plays a significant role. A false negative diagnosis made off an MRI scan could lead the neurologist and patient down an incorrect path and delay an accurate diagnosis, or potentially miss it entirely.
While MRI is not the only piece in the puzzle for MS diagnosis, it plays a significant role. A false negative diagnosis made off an MRI scan could lead the neurologist and patient down an incorrect path and delay an accurate diagnosis, or potentially miss it entirely.
The positive findings on Malcolm’s exam and his new report provide additional essential information for his neurologist, allowing him (the neurologist) to combine these imaging findings with other test results and physical exam findings to come to an accurate diagnosis.
I would always suggest patients seek a second opinion for complex medical diagnoses, especially if the patient feels that something is being missed or that their concerns aren’t being addressed. This could mean setting up an appointment with a second neurologist or submitting your radiology exams for a second opinion to a company such as DocPanel, where they will be interpreted by subspecialty trained and certified neuroradiologists. I personally like to explain the imaging findings in layman’s terms, to ensure that the patient understands the disease process. I believe this empowers patients so that they can take an active role in ensuring the best decisions regarding their care are made.
[Malcolm] After a few months of working with my current neurologist and a support group of people diagnosed with MS, I have found that the most important thing people in my shoes can do is be your own advocate. MS is such an odd, and individual disease. No two patients are exactly alike in their presentation or their symptoms. This can make it very difficult to diagnose. It is always helpful to get several opinions; your health is just to darn important.
DocPanel is committed to making sure every patient receives excellent care. If you would like an expert second opinion on your medical imaging scan from Dr.Rozenfeld or one of our other neuroradiology subspecialists, you can learn morehere.
Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA Woo-Suk Chung, M.D.1 , Tae-Sub Chung, M.D.1 , Hyung Jung Kim, M.D.2 , Chul Min Ahn, M.D.2 , Jae Hoon Lee, M.D.1 , Jin Hur, M.D.1 , Arthur Eung-Hyuck Cho, M.D.1 Purpose : Early detection of small brain metastases is important.
The purpose of this study was to compare the detectability of brain metastases according to the size between 1.5 T and 3.0 T MRI. Materials and Methods :
We reviewed 162 patients with primary lung cancer who were examined for TNM staging. After administration of double dose of Gd-DTPA, MR imaging was performed with SPGR by 3.0 T MRI and then with T1 SE sequence by 1.5 T MRI. In each patient, three readers performed qualitative assessment. Sensitivity, positive predictive value, and diagnostic accuracy were calculated in 3.0 T and 1.5 T MRI according to size. Using the signal intensity (SI) measurements between the metastatic nodules and adjacent tissue, nodule-to-adjacent tissue SI ratio was calculated. Results : Thirty-one of 162 patients had apparent metastatic nodules in the brain at either 1.5 T or 3.0 T MR imaging. 143 nodules were detected in 3.0 T MRI, whereas 137 nodules were detected at 1.5 T MRI. Six nodules, only detected in 3.0 T MRI, were smaller than 3.0 mm in dimension. Sensitivity, positive predictive value, and diagnostic accuracy in 3.0 T MRI were 100 %, 100 %, and 100 % respectively, and in 1.5 T MRI were 95.8 %, 88.3 %, and 85.1 % respectively. SI ratio was significantly higher in the 3.0 T MRI than 1.5 T MRI (p=0.025). Conclusion : True positive rate of 3.0 T MRI with Gd-DTPA was superior to 1.5 T MRI with Gd-DTPA in detection of metastatic nodules smaller than 3.0 mm. Index words :Magnetic resonance (MR), high-field-strength imaging Brain neoplasm, metastases Contrast medium Introduction Brain metastases present a poor prognosis suggesting a shortened survival time. Early diagnosis of brain involvement and determination of the number of metastases are important not only for quality of life but also for cost effectiveness (1-3).
The decision regarding a conservative versus a surgical approach depends on the number of brain metastases detected by radiologic means (1-3). A contrast-enhanced MRI has become the method of choice for visualization of brain metastases (1). High[1]dose gadolinium-enhanced MR examinations may have advantages over 0.1 mmol/kg examinations in detecting early and/or small metastases (3-7).
A delayed study can also increase the contrast (2). Comparing to the 1.5 T MRI with an axial T1-weighted spin echo sequence (SE), the higher field strength MR systems combined with a sequence of SPGR (spoiled gradient recalled acquisition in the steady state) and administration of a high dose of Gd-DTPA (gadopentetate dimeglumine) may also have advantages in detecting small metastases, although this has not yet been verified by clinical data. The purpose of this study is to compare the detectability of brain metastases classified according to the size of nodules, between thin slice SPGR of 3.0 T and conventional thick slice SE of 1.5 T MRI with the administration of a double dose of Gd[1]DTPA.
Materials and Methods Patients From December 2002 to February 2004, a total of 162 consecutive patients with primary lung cancer participated in our study.
The institutional review board approved our study, and informed consent was obtained from all patients regarding the potential risks of both the double dose of contrast medium and two assessments by MRI scanning on a 3.0 T and 1.5 T machine. After the study, 31 patients of this population were diagnosed as having brain metastases. Mean patient age was 61.2 (range, 43 to 80 years). Protocol On the 3.0 T MR scanner (GE Signa VH/i; GE medical system, Milwaukee, USA), the images were acquired using a standard head coil and an actively shielded gradient system with a maximum gradient strength of 43 mT/m. On the 1.5 T MR scanner (Magnetom Vision; Siemens Medical Systems, Erlangen, Germany), a standard head coil and a maximum gradient strength of 25 mT/m were used. All patients were examined after administrating a contrast agent with a double dose of Gd-DTPA (0.2 mmol/kg). First, examinations were performed on a 3.0 T MR scanner and then were subsequently performed on a 1.5 T MR scanner without additional contrast injection.
The scan interval between the 3.0 T and 1.5 T MR examination was less than 20 minutes. The contrast agent used was Gd-DTPA (Magnevist; Schering AG, Berlin, Germany). In all patients, the double dose of Gd-DTPA at 0.2 mmol/kg was administered intravenously as a bolus and scanning commenced immediately. MR imaging included the following sequences on both scanners:
At 3.0 T MRI, an axial 3D SPGR, which is usually used at present, was used (TR/TE/TI = 5.7/1.44/400 milliseconds; flip angle 20°; 2 mm slice thickness; FOV of 220 mm; matrix size of 512×512 ZIP; spatial resolution of 0.43×0.43×2 mm; two acquisition) with a scan time of 3 minutes 30 seconds. At 1.5 T MRI, an axial T1-weighted spin echo sequence was used (TR/RE = 600/14 milliseconds; flip angle 90°; 5 mm slice thickness; FOV of 210 mm; matrix size of 174×256; spatial resolution of 1.2×0.82×5 mm; two acquisition) with a scan time of 5 minutes 30 seconds.
Three radiologists performed randomized, independent blinded review. The three readers were merely informed that all of the patients had lung malignancies. The postcontrast MR examinations of the brain on all of the patients were evaluated. The readers did not have access to other image sets within each study. The presence, size, and number of metastatic nodules were assessed. The postcontrast images were divided into the following two groups: 3.0 T MRI with a double dose of Gd-DTPA and 1.5 T MRI with a double dose of Gd-DTPA. The readers were asked to document the number of nodules. Each nodule in each study was numbered and classified according to its largest diameter measurement: ≤3 mm, 3 mm to 5 mm, or >5 mm. Woo-Suk Chung et al – 102 – Subsequently, if there was any debate about nodule classification, a final interpretation using imaging studies was done until consensus among the readers was accomplished. If disagreements persisted, 3-6 months of follow-up MR scans were obtained for further validation.
For the patients who had follow-up MR scans, these scans were considered positive for metastases if there was a response to the treatment or if there was a growth of nodules identified during the follow-up period. In addition, the sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of the 3.0 T and 1.5 T MRI were calculated using the results from the final interpretation according to size. A quantitative image assessment was performed next. The same lesions on scans of the two different MRI systems were determined by comparing peripheral structures. Signal intensities of adjacent tissue and nodule were assessed by region of interest (ROI) measurements placed identically on both series of images using the same sized circular ROI from the software available on both scanners. Nodule-to[1]adjacent tissue contrast (SI ratio) is defined by SI ratio = ×100 Stissue1 taken as the signal intensity of an ROI assessed over a nodule and Stissue2 taken as the signal intensity assessed over the contralateral white matter.
The signal intensity of a nodule was measured within an enhanced area. In inhomogeneously enhanced nodules, the area of maximum uptake was chosen for measurement. Statistical Analysis The paired Wilcoxon’s signed ranks test was used to compare qualitative scores, and the matched-pair-t test was used to compare nodule SI ratios between the 3.0 T and 1.5 T MRI with a double dose of Gd-DTPA. For all tests, significance was set at p < 0.05, and SPSS software (SPSS Inc. Chicago, US) was used for statistical analyses. Results In the final review made by consensus of three radiologists (Table 1), a total of 143 metastatic nodules were detected by the 3.0 T MRI with a double dose of Gd-DTPA. Of these nodules, 49 nodules were ≤ 3 mm in diameter, 37 nodules were 3 mm to 5 mm, and 57 nodules were >5 mm. A total of 137 metastatic nodules were detected by the 1.5 T MRI with a double dose of Gd-DTPA in the final interpretation. Of these nodules, 43 nodules were ≤ 3 mm in diameter. The 3.0 T MRI with a double dose of Gd-DTPA was significantly more effective at detecting nodules smaller than 3 mm (p = 0.014) than the 1.5 T MRI. However, we found no significant difference in the detection of nodules larger than 3 mm (p > 0.05) (Table 1). In 6 of the 31 cases, six nodules, which were only detected by the 3.0 T MRI with a double dose of Gd[1]DTPA, and missed by the 1.5 T MRI with a double dose of Gd-DTPA, were unanimously agreed upon by all participants in the final interpretation. In three of the six nodules, a growing nodule was detected during a follow-up MR scan which confirmed the presence of metastases (Fig. 1). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of Gd-DTPA due to artifact (Fig. 2). Finally the 3.0 T MRI with a double dose of Gd-DTPA was Stissue1 – Stissue2 Stissue2 Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA – 103 – Table 1. Total Number of Brain Metastases Classified by Size and Detected at the Final Interpretation Size 3.0 T MRI with 1.5 T MRI with p value Gd-DTPA Gd-DPTA ≤ 3 mm 49 43 0.014 3 mm<-≤5 mm 37 37 > 0.05 5 mm< 57 57 > 0.05 Total 143 137 0.014 Note : Data are the number of nodules Table 2. The Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRIs with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm Present Absent Present Absent 3.0 T MRI with Positive 143 00* 49 0* Gd-DTPA Negatiive 000 00* 00 0* 1.5 T MRI with Positive 137 18* 43 18* Gd-DTPA Negative 006 00* 06 0* * Pseudolesions that were detected as nodules by the 1.5 T MRI were detected as vascular structures by the 3.0 T MRI. useful for confirming the presence of these nodules. Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter or better delineation than by the 1.5 T MRI with a double dose of Gd-DTPA. Out of 137 nodules, 65 were brighter (Fig. 3) and out of 137 nodules, 63 were better delineated (Fig. 4). Forty[1]five of 137 nodules were satisfactory in both conditions. By consensus, the final review stated, nodules detected by the 3.0 T and 1.5 T MRI were considered positive for metastases (Table 2). Additionally, there were 18 pseudolesions which were detected as nodules by the 1.5 T MRI, but as vascular structures by the 3.0 T MRI (Fig. 5). The sensitivity, positive predictive values, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 95.8%, 88.3%, and 85.1% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of the 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and Woo-Suk Chung et al – 104 – a b Fig. 2.
A 73-year-old male with multiple brain metastases. Metastatic nodule (a) by a 3.0 T MR image with a double dose of Gd-DTPA show a metastatic nodule (arrow). But (b) the 1.5 T MR image with a double dose of Gd-DTPA cannot show the metastatic nodule by artifact. abc Fig. 1. A 65-year-old male with single brain metastasis. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a small metastatic nodule (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA cannot show the nodule. In (c), a growing nodule was detected during the follow-up MRI with a double dose of Gd-DTPA which confirmed the presence of metastasis (arrow). 100% respectively. For metastatic nodules smaller than 3 mm, the sensitivity, positive predictive value, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 87.8%, 70.5%, and 64.2% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and 100% respectively (Table 3). For quantitative image assessment, the SI ratio in the post contrast sequences (Table 4) was significantly higher in the 3.0 T MRI with a double dose of Gd[1]DTPA than in the 1.5 T MRI with a double dose of Gd[1]DTPA (p = 0.025). Discussion Detection of metastatic nodules is dependent on both their size and contrast ratio (2). As methods to increase the contrast, a higher dose of Gd-DTPA, a higher field strength, and delayed study can all be used to aid detection (2-5, 8-17). Nodules larger than 10 mm are easily detected because vasogenic edema is customarily associated with larger metastases (2). So, when a higher dose of Gd-DTPA is used, the detection rate of larger nodules is not influenced. However, a higher dose is helpful for detecting small nodules because it increases nodule enhancement, yet this method has the disadvantages of increasing the false positive rate and promoting side effects (2-5, 8-14).
A delayed study can also increase the contrast (2). It has been recommended that image acquisition be delayed from 5 to 35 minutes after the administration of contrast material at a dose of 0.1 mmol/kg to ensure optimal detection (2, 15). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of Gd[1]DTPA due to partial volume artifact. Eighteen lesions were detected in the 1.5 T MRI with a double dose of Gd-DTPA, which proved to be vascular structures in 3.0 T MRI with a double dose of Gd- DTPA. The true nature of these lesions was revealed because of the greater morphologic detail visualized by the high field Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA – 105 – a b Fig. 3. A 65-year-old male with multiple brain metastases. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhancement (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhance[1]ment (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter than when observed by the 1.5 T MRI with a double dose of Gd[1]DTPA. Table 3. Estimation of the Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRI with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm 3.0 T 1.5T 3.0 T 1.5T Sensitivity 100 95.8 100 87.8 Specificity – 0 – 0 Positive predictive value 100 88.3 100 70.5 Negative predictive value – 0 – 0 Diagnostic accuracy 100 85.1 100 64.2 Table 4. Results of a quantitative assessment of nodules that were detected by the 3.0 T and 1.5 T MRIs with Gd-DTPA (n=137) 3.0 T 1.5 T P value Nodules-to-adjacent tissue: SI ratio 94.59 63.86 0.025 strength MR image, thus allowing differentiation between true enhancing lesions and sulcal vessels. In our study, each nodules was classified according to its largest diameter as being ≤ 3 mm, 3 mm to 5 mm, and >5 mm because the slice thickness of the 3.0 T MRI was 2.0 mm and 5 mm for the 1.5 T MRI. Therefore this study classified small metastatic nodules as being smaller than 3 mm. Although our study supports the use of a higher field strength MRI with a double dose of Gd-DTPA for increased metastatic nodule detection and for improved nodule enhancement and delineation, the results should be interpretated with caution.
The reason for this is that for patients with two or more brain metastases, additional metastases found with the 3.0 T MRI seem to be of limited clinical importance. The presence of two or more small nodules generally will not change the way the patient is managed. Therefore, it is of utmost importance to identify the difference between none, one, and more than one metastatic nodule.
Patients with a single metastatic nodule located in a respectable region can be treated surgically, and the tumor staged as M1, not M0. However, patients with two or more metastatic nodules are usually Woo-Suk Chung et al – 106 – a b Fig. 5. A 67-year-old female with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows vascular structure (arrow). (b) The 1.5 T MRI with a double dose of Gd[1]DTPA shows a nodular lesion (arrow). A pseudolesion that was detected as a nodule by the 1.5 T MRI with a double dose of Gd[1]DTPA but as a vascular structure by the 3.0 T MRI with a double dose of Gd-DTPA is showed in this figure. a b Fig. 4. A 64-year-old male with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows a metastatic nodule with ring enhancement (arrow). (b) The 1.5 T MRI with Gd-DTPA show a metastatic nodule with ring enhancement (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were better delineated than when observed by the 1.5 T MRI with a double dose of Gd[1]DTPA. treated with radiation therapy and/or systemic chemotherapy (3, 18-22). On the other hand, the use of a higher strength field MRI was found to be helpful in confirming the appearance of an equivocal metastatic nodule. The 3.0 T MRI with a double dose of Gd-DTPA was also useful for the detection of additional metastases in patients with a known lesion detected by the 1.5 T MRI with a double dose of Gd[1]DTPA. Because this also has influence on the sensitivity, positive predictive value, and diagnostic accuracy the 3.0 T MRI with a double dose of Gd[1]DTPA was found to have better results than the 1.5 T MRI with a double dose of Gd-DTPA in our study. Therefore we recommend the use of the 3.0 T MRI with a double dose of Gd-DTPA in only three circumstances: when the findings by the 1.5 T MRI with Gd-DTPA are equivocal, when one potentially surgically respectable nodule is identified, or for detecting early and/or small metastases
There were two limitations in this study. The first limitation was a difference in protocol sequence. The T1 weighted spin-echo protocol was used for the 1.5 T MRI and SPGR technique protocol for the 3.0 T MRI. Detectability of metastatic nodules is more effective with 3.0 T MRI with T1 SE than with a 1.5 T MRI with SE (2). SPGR with thin slice thickness is superior to the T1 spin echo sequence with thick slice thickness due to a partial volume effect. Additionally, SE is not optimum for a 3.0 T due to longer T1- and shorter T2- relaxation times of water protons, which decrease the contrast ratio in the 3.0 T images.17 The purpose of this study was to detect early small brain metastases, so using the SPGR sequence with a 3.0 T MRI, which is usually used at present, has advantages for detecting early small brain metastases. The second limitation was that the scan interval between the 1.5 T and 3.0 T MRI was less than 20 minutes. However, a delayed study increases contrast as mentioned above. The current study found that the SI ratio was significantly higher in the 3.0T images than in the 1.5 T images. Considering the delayed study by the 1.5 T MRI, this limitation emphasizes the better detection rate of the 3.0 T MRI with a double dose of Gd-DTPA. And due to these confounding variables, blinded reviews were performed by three readers. The detectability of metastatic nodules smaller than 3mm was better using a 3.0 T MRI with SPGR than a 1.5 T MRI with T1 SE. Therefore we recommend a 3.0 T MRI with SPGR and a double dose of Gd-DTPA for detecting early and/or small metastatic nodules, furthermore influencing treatment. References 1.Lassman AB, DeAngelis LM. Brain metastases. Neurol Clin. 2003; 21:1-23, vii, Review 2.Ba-Ssalamah A, Nobauer-Huhmann IM, Pinker K, et al. Effect of contrast dose and field strength in the magnetic resonance detection of brain metastases. Invest Radiol 2003; 38: 415-422 3.Sze G, Johnson C, Kawamura Y, et al. Comparison of single[1]and triple-dose contrast material in the MR screening of brain metastases. AJNR Am J Neuroradiol 1998; 19:821-828 4.Runge VM, Kirsch JE, Burke VJ, et al. High-dose Gadoteridol in MR imaging of intracranial neoplasm. J Magn Reson Imaging 1992; 2:9-18 5.Yuh WT, Engelken JD, Muhonen MG, Mayr NA, Fisher DJ, Ehrhardt JC. Experience with high-dose gadolinium MR imaging in the evaluation of brain metastases. AJNR Am J Neuroradiol 1992; 13:335-345 6.Brekenfeld C, Foert E, Hundt W, Kenn W, Lodeann KP, Gehl HB. Enhancement of cerebral diseases: How much contrast agent is enough? Comparison of 0.1, 0.2, and 0.3 mmol/kg Gadoteridol at 0.2 T with 0.1 mmol/kg Gadoteridol at 1.5 T. Invest Radiol 2001; 36:266-275 7.Yuh WT, Tali ET, Nguyen HD, Simonson TM, Mayr NA, Fisher DJ. The effect of contrast dose, imaging time, and lesion size in the MR detection of intracerebral metastasis. AJNR Am J Neuroradiol 1998; 16:373-380 8.Van Dijk P, Sijens PE, Schmitz PI, Oudkerk M. Gd-enhanced MR imaging of brain metastases: contrast as a function of dose and lesion size. Magn Reson Imaging 1997; 15:535-541 9.Yuh WT, Fisher DJ, Engelken JD, et al. MR evaluation of CNS tumors: dose comparison study with gadopentetate dimeglumine and gadoteridol. Radiology 1991; 180:485-491 10.Healy ME, Hasselink JR, Press GA, Middleton MS. Increased detection of intracranial metastases with intravenous Gd[1]DTPA. Radiology 1987; 165:619-624 11.Akeson P, Vikhoff B, Stahlberg F, Holtas S. Brain lesion contrast in MR imaging: dependence of field strength and concentration of gadodiamide injection in patients and phantoms. Acta Radiol 1977; 38:14-18 12.Runge VM. A review of contrast media research in 1999 – 2000. Invest Radiol 2001; 36:123-130 13.Yuh WT, Parker JR Carvlin MJ. Indication related dosing for magnetic resonance contrast media. Eur Radiol 1977; 7(suppl 5):S269-S275 14.Rinck PA, Muller RN. Field strength and dose dependence of contrast enhancement by Gadolinium-based MR contrast agents. Eur Radiol 1999; 9:998-1004 15.Schorner W, Laniado M, Niendorf HP, Schubert C, Felix R. Time-dependent changes in image contrast in brain tumors after gadolinium-DTPA. AJNR Am J Neuroradiol 1986; Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA – 107 – 7:1013-1020 16.Chang KH, Ra DG, Han MH, Cha SH, Kim HD, Han MC. Contrast enhancement of brain tumors at different MR field strengths: comparison of 0.5 T and 2.0 T. AJNR Am J Neuroradiol 1994; 15:1413-1419 17.Nobauer-Huhmann IM, Ba-Ssalamah A, Mlynarik V, et al. Magnetic resonance imaging contrast enhancement of brain tumors at 3 tesla versus 1.5 tesla. Invest Radiol 2002; 37:114- 119 18.Galicich JH, Sundaresan N, Thaler HT. Surgical treatment of single brain metastasis: evaluation of results by computerized tomography scanning. J Neurosurg 1980; 53:63-67 19.Runge VM, Carollo BR, Wolf CR, Nelson KL, Gelblum DY. Gd-DTPA: A review of clinical indications in central nervous system magnetic resonance imaging. Radiographics 1989; 9:929-958 20.Earnest F 4th, Ryu JH, Miller GM, et al. Suspected non-small cell lung cancer: Incidence of occult brain and skeletal metastases and effectiveness of imaging for detection-Pilot study. Radiology 1999; 211:137-145 21.Koutras AK, Marangos M, Kourelis T, et al. Surgical management of cerebral metastases from non-small cell lung cancer. Tumori 2003; 89:292-297 22.Soffietti R, Ruda R, Mutani R. Management of brain metastases. J Neurol 2002; 249:1357-1369. Review Woo-Suk Chung et al – 108 – 통신저자 : 정태섭, 서울특별시 강남구 도곡동 146-92 연세대학교 영동세브란스병원 영상의학과 Tel. 82-2019-3514 Fax. 82-3462-5472 E-mail: tschung@yumc.yonsei.ac.kr 뇌전이종양의발견에있어서Doble dose Gd-DTPA를이용한 3 T MRI와1.5 T MRI간의비교연구 1 연세대학교 영동세브란스병원 영상의학과 2 연세대학교 영동세브란스병원 호흡기내과 정우석1 ·정태섭1 ·김형중2 ·안철민2 ·이재훈1 ·허 진1 ·조응혁1 목적: 작은 뇌전이 종양의 조기 발견은 중요하다. 이 연구의 목적은 1.5 T MRI와 3.0 T MRI 간의 크기에 따른 뇌 전이 종양의 발견율을 비교하는 것이다. 대상 및 방법: 폐암으로 진단 받은 162명의 환자를 대상으로 TNM 병기를 위해 뇌 MRI를 시행하였다. Gd-DTPA 를 2배 용량으로 투여 후, 3.0 T MRI에서 훼손경사회복획득으로 촬영하였으며 그 후 1.5 T MRI에서 T1 스핀 에 코로 촬영하였다. 3명의 방사선과 전문의가 합의하여 MRI를 판독하였으며 정성 평가를 시행하였다. 3.0 T와 1.5 T MRI에서 크기에 따라 민감도, 양성 예측률, 정확도를 평가하였다. 신호 강도를 사용하여 전이 종양과 인접 조직간 의 신호강도 비를 계산하였다. 결과: 162명의 환자 중 31명에서 1.5 T 또는 3.0 T MR에 뇌전이 종양이 발견되었다. 3.0 T MRI에서 143개의 종 양이 발견되었으나 1.5 T MRI에서 137개의 종양이 발견되었다. 6개의 종양이 3.0 T MRI에서만 발견되었으며 크 기는 모두 3 mm 미만이었다. 3.0 T MRI의 민감도, 양성 예측률, 정확도는 각각 100%, 100%, 100%이며, 1.5 T MRI에서는 각각 95.8%, 88.3%, 85.1% 이다. SI ratio는 1.5 T MRI보다 3.0 T MRI에서 유의하게 높았다 (p=0.025). 결론: Double dose Gd-DTPA를 이용한 3.0 T MRI는 3 mm미만의 뇌전이 종양을 발견하는데 있어서 1.5 T
Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA Woo-Suk Chung, M.D.1 , Tae-Sub Chung, M.D.1 , Hyung Jung Kim, M.D.2 , Chul Min Ahn, M.D.2 , Jae Hoon Lee, M.D.1 , Jin Hur, M.D.1 , Arthur Eung-Hyuck Cho, M.D.1 Purpose : Early detection of small brain metastases is important. The purpose of this study was to compare the detectability of brain metastases according to the size between 1.5 T and 3.0 T MRI. Materials and Methods : We reviewed 162 patients with primary lung cancer who were examined for TNM staging. After administration of double dose of Gd-DTPA, MR imaging was performed with SPGR by 3.0 T MRI and then with T1 SE sequence by 1.5 T MRI. In each patient, three readers performed qualitative assessment. Sensitivity, positive predictive value, and diagnostic accuracy were calculated in 3.0 T and 1.5 T MRI according to size. Using the signal intensity (SI) measurements between the metastatic nodules and adjacent tissue, nodule-to-adjacent tissue SI ratio was calculated. Results : Thirty-one of 162 patients had apparent metastatic nodules in the brain at either 1.5 T or 3.0 T MR imaging. 143 nodules were detected in 3.0 T MRI, whereas 137 nodules were detected at 1.5 T MRI. Six nodules, only detected in 3.0 T MRI, were smaller than 3.0 mm in dimension. Sensitivity, positive predictive value, and diagnostic accuracy in 3.0 T MRI were 100 %, 100 %, and 100 % respectively, and in 1.5 T MRI were 95.8 %, 88.3 %, and 85.1 % respectively. SI ratio was significantly higher in the 3.0 T MRI than 1.5 T MRI (p=0.025). Conclusion : True positive rate of 3.0 T MRI with Gd-DTPA was superior to 1.5 T MRI with Gd-DTPA in detection of metastatic nodules smaller than 3.0 mm. Index words :Magnetic resonance (MR), high-field-strength imaging Brain neoplasm, metastases Contrast medium Introduction Brain metastases present a poor prognosis suggesting a shortened survival time. Early diagnosis of brain involvement and determination of the number of metastases are important not only for quality of life but also for cost effectiveness (1-3). The decision regarding a conservative versus a surgical approach depends on the number of brain metastases detected by radiologic means (1-3). A contrast-enhanced MRI has become the method of choice for visualization of brain metastases (1). Highdose gadolinium-enhanced MR examinations may have advantages over 0.1 mmol/kg examinations in detecting early and/or small metastases (3-7). A delayed study can also increase the contrast (2). Comparing to the 1.5 T MRI with an axial T1-weighted spin echo sequence (SE), the higher field strength MR systems combined with a sequence of SPGR (spoiled gradient recalled acquisition in the steady state) and administration of a high dose of Gd-DTPA (gadopentetate dimeglumine) may also have advantages in detecting small metastases, although this has not yet been verified by clinical data. The purpose of this study is to compare the detectability of brain metastases classified according to the size of nodules, between thin slice SPGR of 3.0 T and conventional thick slice SE of 1.5 T MRI with the administration of a double dose of GdDTPA. Materials and Methods Patients From December 2002 to February 2004, a total of 162 consecutive patients with primary lung cancer participated in our study. The institutional review board approved our study, and informed consent was obtained from all patients regarding the potential risks of both the double dose of contrast medium and two assessments by MRI scanning on a 3.0 T and 1.5 T machine. After the study, 31 patients of this population were diagnosed as having brain metastases. Mean patient age was 61.2 (range, 43 to 80 years). Protocol On the 3.0 T MR scanner (GE Signa VH/i; GE medical system, Milwaukee, USA), the images were acquired using a standard head coil and an actively shielded gradient system with a maximum gradient strength of 43 mT/m. On the 1.5 T MR scanner (Magnetom Vision; Siemens Medical Systems, Erlangen, Germany), a standard head coil and a maximum gradient strength of 25 mT/m were used. All patients were examined after administrating a contrast agent with a double dose of Gd-DTPA (0.2 mmol/kg). First, examinations were performed on a 3.0 T MR scanner and then were subsequently performed on a 1.5 T MR scanner without additional contrast injection. The scan interval between the 3.0 T and 1.5 T MR examination was less than 20 minutes. The contrast agent used was Gd-DTPA (Magnevist; Schering AG, Berlin, Germany). In all patients, the double dose of Gd-DTPA at 0.2 mmol/kg was administered intravenously as a bolus and scanning commenced immediately. MR imaging included the following sequences on both scanners: At 3.0 T MRI, an axial 3D SPGR, which is usually used at present, was used (TR/TE/TI = 5.7/1.44/400 milliseconds; flip angle 20°; 2 mm slice thickness; FOV of 220 mm; matrix size of 512×512 ZIP; spatial resolution of 0.43×0.43×2 mm; two acquisition) with a scan time of 3 minutes 30 seconds. At 1.5 T MRI, an axial T1-weighted spin echo sequence was used (TR/RE = 600/14 milliseconds; flip angle 90°; 5 mm slice thickness; FOV of 210 mm; matrix size of 174×256; spatial resolution of 1.2×0.82×5 mm; two acquisition) with a scan time of 5 minutes 30 seconds. Three radiologists performed randomized, independent blinded review. The three readers were merely informed that all of the patients had lung malignancies. The postcontrast MR examinations of the brain on all of the patients were evaluated. The readers did not have access to other image sets within each study. The presence, size, and number of metastatic nodules were assessed. The postcontrast images were divided into the following two groups: 3.0 T MRI with a double dose of Gd-DTPA and 1.5 T MRI with a double dose of Gd-DTPA. The readers were asked to document the number of nodules. Each nodule in each study was numbered and classified according to its largest diameter measurement: ≤3 mm, 3 mm to 5 mm, or
5 mm. Woo-Suk Chung et al
102 – Subsequently, if there was any debate about nodule classification, a final interpretation using imaging studies was done until consensus among the readers was accomplished. If disagreements persisted, 3-6 months of follow-up MR scans were obtained for further validation. For the patients who had follow-up MR scans, these scans were considered positive for metastases if there was a response to the treatment or if there was a growth of nodules identified during the follow-up period. In addition, the sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of the 3.0 T and 1.5 T MRI were calculated using the results from the final interpretation according to size. A quantitative image assessment was performed next. The same lesions on scans of the two different MRI systems were determined by comparing peripheral structures. Signal intensities of adjacent tissue and nodule were assessed by region of interest (ROI) measurements placed identically on both series of images using the same sized circular ROI from the software available on both scanners. Nodule-toadjacent tissue contrast (SI ratio) is defined by SI ratio = ×100 Stissue1 taken as the signal intensity of an ROI assessed over a nodule and Stissue2 taken as the signal intensity assessed over the contralateral white matter. The signal intensity of a nodule was measured within an enhanced area. In inhomogeneously enhanced nodules, the area of maximum uptake was chosen for measurement. Statistical Analysis The paired Wilcoxon’s signed ranks test was used to compare qualitative scores, and the matched-pair-t test was used to compare nodule SI ratios between the 3.0 T and 1.5 T MRI with a double dose of Gd-DTPA. For all tests, significance was set at p < 0.05, and SPSS software (SPSS Inc. Chicago, US) was used for statistical analyses. Results In the final review made by consensus of three radiologists (Table 1), a total of 143 metastatic nodules were detected by the 3.0 T MRI with a double dose of Gd-DTPA. Of these nodules, 49 nodules were ≤ 3 mm in diameter, 37 nodules were 3 mm to 5 mm, and 57 nodules were >5 mm. A total of 137 metastatic nodules were detected by the 1.5 T MRI with a double dose of Gd-DTPA in the final interpretation. Of these nodules, 43 nodules were ≤ 3 mm in diameter. The 3.0 T MRI with a double dose of Gd-DTPA was significantly more effective at detecting nodules smaller than 3 mm (p = 0.014) than the 1.5 T MRI. However, we found no significant difference in the detection of nodules larger than 3 mm (p > 0.05) (Table 1). In 6 of the 31 cases, six nodules, which were only detected by the 3.0 T MRI with a double dose of GdDTPA, and missed by the 1.5 T MRI with a double dose of Gd-DTPA, were unanimously agreed upon by all participants in the final interpretation. In three of the six nodules, a growing nodule was detected during a follow-up MR scan which confirmed the presence of metastases (Fig. 1). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of Gd-DTPA due to artifact (Fig. 2). Finally the 3.0 T MRI with a double dose of Gd-DTPA was Stissue1 – Stissue2 Stissue2 Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA
103 – Table 1. Total Number of Brain Metastases Classified by Size and Detected at the Final Interpretation Size 3.0 T MRI with 1.5 T MRI with p value Gd-DTPA Gd-DPTA ≤ 3 mm 49 43 0.014 3 mm<-≤5 mm 37 37 > 0.05 5 mm< 57 57 > 0.05 Total 143 137 0.014 Note : Data are the number of nodules Table 2. The Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRIs with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm Present Absent Present Absent 3.0 T MRI with Positive 143 00* 49 0* Gd-DTPA Negatiive 000 00* 00 0* 1.5 T MRI with Positive 137 18* 43 18* Gd-DTPA Negative 006 00* 06 0*
Pseudolesions that were detected as nodules by the 1.5 T MRI were detected as vascular structures by the 3.0 T MRI. useful for confirming the presence of these nodules. Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter or better delineation than by the 1.5 T MRI with a double dose of Gd-DTPA. Out of 137 nodules, 65 were brighter (Fig. 3) and out of 137 nodules, 63 were better delineated (Fig. 4). Fortyfive of 137 nodules were satisfactory in both conditions. By consensus, the final review stated, nodules detected by the 3.0 T and 1.5 T MRI were considered positive for metastases (Table 2). Additionally, there were 18 pseudolesions which were detected as nodules by the 1.5 T MRI, but as vascular structures by the 3.0 T MRI (Fig. 5). The sensitivity, positive predictive values, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 95.8%, 88.3%, and 85.1% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of the 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and Woo-Suk Chung et al
104 – a b Fig. 2. A 73-year-old male with multiple brain metastases. Metastatic nodule (a) by a 3.0 T MR image with a double dose of Gd-DTPA show a metastatic nodule (arrow). But (b) the 1.5 T MR image with a double dose of Gd-DTPA cannot show the metastatic nodule by artifact. abc Fig. 1. A 65-year-old male with single brain metastasis. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a small metastatic nodule (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA cannot show the nodule. In (c), a growing nodule was detected during the follow-up MRI with a double dose of Gd-DTPA which confirmed the presence of metastasis (arrow). 100% respectively. For metastatic nodules smaller than 3 mm, the sensitivity, positive predictive value, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 87.8%, 70.5%, and 64.2% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and 100% respectively (Table 3). For quantitative image assessment, the SI ratio in the post contrast sequences (Table 4) was significantly higher in the 3.0 T MRI with a double dose of GdDTPA than in the 1.5 T MRI with a double dose of GdDTPA (p = 0.025). Discussion Detection of metastatic nodules is dependent on both their size and contrast ratio (2). As methods to increase the contrast, a higher dose of Gd-DTPA, a higher field strength, and delayed study can all be used to aid detection (2-5, 8-17). Nodules larger than 10 mm are easily detected because vasogenic edema is customarily associated with larger metastases (2). So, when a higher dose of Gd-DTPA is used, the detection rate of larger nodules is not influenced. However, a higher dose is helpful for detecting small nodules because it increases nodule enhancement, yet this method has the disadvantages of increasing the false positive rate and promoting side effects (2-5, 8-14). A delayed study can also increase the contrast (2). It has been recommended that image acquisition be delayed from 5 to 35 minutes after the administration of contrast material at a dose of 0.1 mmol/kg to ensure optimal detection (2, 15). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of GdDTPA due to partial volume artifact. Eighteen lesions were detected in the 1.5 T MRI with a double dose of Gd-DTPA, which proved to be vascular structures in 3.0 T MRI with a double dose of Gd- DTPA. The true nature of these lesions was revealed because of the greater morphologic detail visualized by the high field Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA
105 – a b Fig. 3. A 65-year-old male with multiple brain metastases. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhancement (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhancement (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter than when observed by the 1.5 T MRI with a double dose of GdDTPA. Table 3. Estimation of the Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRI with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm 3.0 T 1.5T 3.0 T 1.5T Sensitivity 100 95.8 100 87.8 Specificity – 0 – 0 Positive predictive value 100 88.3 100 70.5 Negative predictive value – 0 – 0 Diagnostic accuracy 100 85.1 100 64.2 Table 4. Results of a quantitative assessment of nodules that were detected by the 3.0 T and 1.5 T MRIs with Gd-DTPA (n=137) 3.0 T 1.5 T P value Nodules-to-adjacent tissue: SI ratio 94.59 63.86 0.025 strength MR image, thus allowing differentiation between true enhancing lesions and sulcal vessels. In our study, each nodules was classified according to its largest diameter as being ≤ 3 mm, 3 mm to 5 mm, and >5 mm because the slice thickness of the 3.0 T MRI was 2.0 mm and 5 mm for the 1.5 T MRI. Therefore this study classified small metastatic nodules as being smaller than 3 mm. Although our study supports the use of a higher field strength MRI with a double dose of Gd-DTPA for increased metastatic nodule detection and for improved nodule enhancement and delineation, the results should be interpretated with caution. The reason for this is that for patients with two or more brain metastases, additional metastases found with the 3.0 T MRI seem to be of limited clinical importance. The presence of two or more small nodules generally will not change the way the patient is managed. Therefore, it is of utmost importance to identify the difference between none, one, and more than one metastatic nodule. Patients with a single metastatic nodule located in a respectable region can be treated surgically, and the tumor staged as M1, not M0. However, patients with two or more metastatic nodules are usually Woo-Suk Chung et al
106 – a b Fig. 5. A 67-year-old female with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows vascular structure (arrow). (b) The 1.5 T MRI with a double dose of GdDTPA shows a nodular lesion (arrow). A pseudolesion that was detected as a nodule by the 1.5 T MRI with a double dose of GdDTPA but as a vascular structure by the 3.0 T MRI with a double dose of Gd-DTPA is showed in this figure. a b Fig. 4. A 64-year-old male with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows a metastatic nodule with ring enhancement (arrow). (b) The 1.5 T MRI with Gd-DTPA show a metastatic nodule with ring enhancement (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were better delineated than when observed by the 1.5 T MRI with a double dose of GdDTPA. treated with radiation therapy and/or systemic chemotherapy (3, 18-22). On the other hand, the use of a higher strength field MRI was found to be helpful in confirming the appearance of an equivocal metastatic nodule. The 3.0 T MRI with a double dose of Gd-DTPA was also useful for the detection of additional metastases in patients with a known lesion detected by the 1.5 T MRI with a double dose of GdDTPA. Because this also has influence on the sensitivity, positive predictive value, and diagnostic accuracy the 3.0 T MRI with a double dose of GdDTPA was found to have better results than the 1.5 T MRI with a double dose of Gd-DTPA in our study. Therefore we recommend the use of the 3.0 T MRI with a double dose of Gd-DTPA in only three circumstances: when the findings by the 1.5 T MRI with Gd-DTPA are equivocal, when one potentially surgically respectable nodule is identified, or for detecting early and/or small metastases There were two limitations in this study. The first limitation was a difference in protocol sequence. The T1 weighted spin-echo protocol was used for the 1.5 T MRI and SPGR technique protocol for the 3.0 T MRI. Detectability of metastatic nodules is more effective with 3.0 T MRI with T1 SE than with a 1.5 T MRI with SE (2). SPGR with thin slice thickness is superior to the T1 spin echo sequence with thick slice thickness due to a partial volume effect. Additionally, SE is not optimum for a 3.0 T due to longer T1- and shorter T2- relaxation times of water protons, which decrease the contrast ratio in the 3.0 T images.17 The purpose of this study was to detect early small brain metastases, so using the SPGR sequence with a 3.0 T MRI, which is usually used at present, has advantages for detecting early small brain metastases. The second limitation was that the scan interval between the 1.5 T and 3.0 T MRI was less than 20 minutes. However, a delayed study increases contrast as mentioned above. The current study found that the SI ratio was significantly higher in the 3.0T images than in the 1.5 T images. Considering the delayed study by the 1.5 T MRI, this limitation emphasizes the better detection rate of the 3.0 T MRI with a double dose of Gd-DTPA. And due to these confounding variables, blinded reviews were performed by three readers. The detectability of metastatic nodules smaller than 3mm was better using a 3.0 T MRI with SPGR than a 1.5 T MRI with T1 SE. Therefore we recommend a 3.0 T MRI with SPGR and a double dose of Gd-DTPA for detecting early and/or small metastatic nodules, furthermore influencing treatment. References 1.Lassman AB, DeAngelis LM. Brain metastases. Neurol Clin. 2003; 21:1-23, vii, Review 2.Ba-Ssalamah A, Nobauer-Huhmann IM, Pinker K, et al. Effect of contrast dose and field strength in the magnetic resonance detection of brain metastases. Invest Radiol 2003; 38: 415-422 3.Sze G, Johnson C, Kawamura Y, et al. Comparison of singleand triple-dose contrast material in the MR screening of brain metastases. AJNR Am J Neuroradiol 1998; 19:821-828 4.Runge VM, Kirsch JE, Burke VJ, et al. High-dose Gadoteridol in MR imaging of intracranial neoplasm. J Magn Reson Imaging 1992; 2:9-18 5.Yuh WT, Engelken JD, Muhonen MG, Mayr NA, Fisher DJ, Ehrhardt JC. Experience with high-dose gadolinium MR imaging in the evaluation of brain metastases. AJNR Am J Neuroradiol 1992; 13:335-345 6.Brekenfeld C, Foert E, Hundt W, Kenn W, Lodeann KP, Gehl HB. Enhancement of cerebral diseases: How much contrast agent is enough? Comparison of 0.1, 0.2, and 0.3 mmol/kg Gadoteridol at 0.2 T with 0.1 mmol/kg Gadoteridol at 1.5 T. Invest Radiol 2001; 36:266-275 7.Yuh WT, Tali ET, Nguyen HD, Simonson TM, Mayr NA, Fisher DJ. The effect of contrast dose, imaging time, and lesion size in the MR detection of intracerebral metastasis. AJNR Am J Neuroradiol 1998; 16:373-380 8.Van Dijk P, Sijens PE, Schmitz PI, Oudkerk M. Gd-enhanced MR imaging of brain metastases: contrast as a function of dose and lesion size. Magn Reson Imaging 1997; 15:535-541 9.Yuh WT, Fisher DJ, Engelken JD, et al. MR evaluation of CNS tumors: dose comparison study with gadopentetate dimeglumine and gadoteridol. Radiology 1991; 180:485-491 10.Healy ME, Hasselink JR, Press GA, Middleton MS. Increased detection of intracranial metastases with intravenous GdDTPA. Radiology 1987; 165:619-624 11.Akeson P, Vikhoff B, Stahlberg F, Holtas S. Brain lesion contrast in MR imaging: dependence of field strength and concentration of gadodiamide injection in patients and phantoms. Acta Radiol 1977; 38:14-18 12.Runge VM. A review of contrast media research in 1999 –
Invest Radiol 2001; 36:123-130 13.Yuh WT, Parker JR Carvlin MJ. Indication related dosing for magnetic resonance contrast media. Eur Radiol 1977; 7(suppl 5):S269-S275 14.Rinck PA, Muller RN. Field strength and dose dependence of contrast enhancement by Gadolinium-based MR contrast agents. Eur Radiol 1999; 9:998-1004 15.Schorner W, Laniado M, Niendorf HP, Schubert C, Felix R. Time-dependent changes in image contrast in brain tumors after gadolinium-DTPA. AJNR Am J Neuroradiol 1986; Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA
107 – 7:1013-1020 16.Chang KH, Ra DG, Han MH, Cha SH, Kim HD, Han MC. Contrast enhancement of brain tumors at different MR field strengths: comparison of 0.5 T and 2.0 T. AJNR Am J Neuroradiol 1994; 15:1413-1419 17.Nobauer-Huhmann IM, Ba-Ssalamah A, Mlynarik V, et al. Magnetic resonance imaging contrast enhancement of brain tumors at 3 tesla versus 1.5 tesla. Invest Radiol 2002; 37:114- 119 18.Galicich JH, Sundaresan N, Thaler HT. Surgical treatment of single brain metastasis: evaluation of results by computerized tomography scanning. J Neurosurg 1980; 53:63-67 19.Runge VM, Carollo BR, Wolf CR, Nelson KL, Gelblum DY. Gd-DTPA: A review of clinical indications in central nervous system magnetic resonance imaging. Radiographics 1989; 9:929-958 20.Earnest F 4th, Ryu JH, Miller GM, et al. Suspected non-small cell lung cancer: Incidence of occult brain and skeletal metastases and effectiveness of imaging for detection-Pilot study. Radiology 1999; 211:137-145 21.Koutras AK, Marangos M, Kourelis T, et al. Surgical management of cerebral metastases from non-small cell lung cancer. Tumori 2003; 89:292-297 22.Soffietti R, Ruda R, Mutani R. Management of brain metastases. J Neurol 2002; 249:1357-1369. Review
Neuro Second Opinion Catches Missed Brain Lesions Suggestive of MS
4/16/20
Malcolm’s brain MRI was initially read as completely normal. Upon getting a second opinion, it was discovered that 22 lesions suggestive of multiple sclerosis had been missed. Here is his story.
[Malcolm] After 18 months of deteriorating health, with a multitude of neurological symptoms, I went to see a neurologist. I was ordered a standard brain MRI to help figure out what was going on. By this time, I had been researching my symptoms for a few months, and, in doing so, had developed a basic understanding of what I was looking for: T2 lesions.
When I received the results from my MRI, the report said everything was normal. I met with my neurologist, and he too said there was nothing abnormal about my scan. When I viewed the MRI myself, however, I found 4 spots that looked to me to be brain lesions. I brought them up to my doctor at my next appointment but was essentially laughed at.
It was quite unsettling to have something so concerning be shrugged off. After that appointment, I decided I wanted to switch to a new neurologist and get a second opinion on my MRI scan. I made an appointment with the new doctor, but it was going to be another 6 weeks before I could be seen. Fortunately, I found DocPanel. I submitted my MRI for review and, within 48 hours, I got my results back.
[Dr. Michael Rozenfeld] Malcolm reached out to DocPanel due to concern for a missed diagnosis. He was reportedly having symptoms suspicious for multiple sclerosis but his MRI was initially read as completely normal. Based on my review of his MRI, the exam was not normal. Malcolm had significant findings that were certainly suggestive of, but not entirely specific for, multiple sclerosis.
[Malcolm] My second opinion results were quite alarming – there were not 4 lesions, but 22. Twenty-two! They were small, but they were most definitely there. I took the second opinion report to my new neurologist, and now I am being considered for possible Primary Progressive Multiple Sclerosis. I am scheduled to get new MRIs in November to confirm or rule out MS and you can be sure I will be sending them to DocPanel for a second look!
I have found that the most important thing people in my shoes can do is be your own advocate. MS is such an odd and individual disease. – Malcolm
[Dr. Michael Rozenfeld] Radiology exams can be misinterpreted for a number of reasons – this is unfortunately not uncommon. While MRI is not the only piece in the puzzle for MS diagnosis, it plays a significant role. A false negative diagnosis made off an MRI scan could lead the neurologist and patient down an incorrect path and delay an accurate diagnosis, or potentially miss it entirely.
While MRI is not the only piece in the puzzle for MS diagnosis, it plays a significant role. A false negative diagnosis made off an MRI scan could lead the neurologist and patient down an incorrect path and delay an accurate diagnosis, or potentially miss it entirely.
The positive findings on Malcolm’s exam and his new report provide additional essential information for his neurologist, allowing him (the neurologist) to combine these imaging findings with other test results and physical exam findings to come to an accurate diagnosis.
I would always suggest patients seek a second opinion for complex medical diagnoses, especially if the patient feels that something is being missed or that their concerns aren’t being addressed. This could mean setting up an appointment with a second neurologist or submitting your radiology exams for a second opinion to a company such as DocPanel, where they will be interpreted by subspecialty trained and certified neuroradiologists. I personally like to explain the imaging findings in layman’s terms, to ensure that the patient understands the disease process. I believe this empowers patients so that they can take an active role in ensuring the best decisions regarding their care are made.
[Malcolm] After a few months of working with my current neurologist and a support group of people diagnosed with MS, I have found that the most important thing people in my shoes can do is be your own advocate. MS is such an odd, and individual disease. No two patients are exactly alike in their presentation or their symptoms. This can make it very difficult to diagnose. It is always helpful to get several opinions; your health is just to darn important.
DocPanel is committed to making sure every patient receives excellent care. If you would like an expert second opinion on your medical imaging scan from Dr.Rozenfeld or one of our other neuroradiology subspecialists, you can learn morehere.
Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA Woo-Suk Chung, M.D.1 , Tae-Sub Chung, M.D.1 , Hyung Jung Kim, M.D.2 , Chul Min Ahn, M.D.2 , Jae Hoon Lee, M.D.1 , Jin Hur, M.D.1 , Arthur Eung-Hyuck Cho, M.D.1 Purpose : Early detection of small brain metastases is important.
The purpose of this study was to compare the detectability of brain metastases according to the size between 1.5 T and 3.0 T MRI. Materials and Methods :
We reviewed 162 patients with primary lung cancer who were examined for TNM staging. After administration of double dose of Gd-DTPA, MR imaging was performed with SPGR by 3.0 T MRI and then with T1 SE sequence by 1.5 T MRI. In each patient, three readers performed qualitative assessment. Sensitivity, positive predictive value, and diagnostic accuracy were calculated in 3.0 T and 1.5 T MRI according to size. Using the signal intensity (SI) measurements between the metastatic nodules and adjacent tissue, nodule-to-adjacent tissue SI ratio was calculated. Results : Thirty-one of 162 patients had apparent metastatic nodules in the brain at either 1.5 T or 3.0 T MR imaging. 143 nodules were detected in 3.0 T MRI, whereas 137 nodules were detected at 1.5 T MRI. Six nodules, only detected in 3.0 T MRI, were smaller than 3.0 mm in dimension. Sensitivity, positive predictive value, and diagnostic accuracy in 3.0 T MRI were 100 %, 100 %, and 100 % respectively, and in 1.5 T MRI were 95.8 %, 88.3 %, and 85.1 % respectively. SI ratio was significantly higher in the 3.0 T MRI than 1.5 T MRI (p=0.025). Conclusion : True positive rate of 3.0 T MRI with Gd-DTPA was superior to 1.5 T MRI with Gd-DTPA in detection of metastatic nodules smaller than 3.0 mm. Index words :Magnetic resonance (MR), high-field-strength imaging Brain neoplasm, metastases Contrast medium Introduction Brain metastases present a poor prognosis suggesting a shortened survival time. Early diagnosis of brain involvement and determination of the number of metastases are important not only for quality of life but also for cost effectiveness (1-3).
The decision regarding a conservative versus a surgical approach depends on the number of brain metastases detected by radiologic means (1-3). A contrast-enhanced MRI has become the method of choice for visualization of brain metastases (1). High[1]dose gadolinium-enhanced MR examinations may have advantages over 0.1 mmol/kg examinations in detecting early and/or small metastases (3-7).
A delayed study can also increase the contrast (2). Comparing to the 1.5 T MRI with an axial T1-weighted spin echo sequence (SE), the higher field strength MR systems combined with a sequence of SPGR (spoiled gradient recalled acquisition in the steady state) and administration of a high dose of Gd-DTPA (gadopentetate dimeglumine) may also have advantages in detecting small metastases, although this has not yet been verified by clinical data. The purpose of this study is to compare the detectability of brain metastases classified according to the size of nodules, between thin slice SPGR of 3.0 T and conventional thick slice SE of 1.5 T MRI with the administration of a double dose of Gd[1]DTPA.
Materials and Methods Patients From December 2002 to February 2004, a total of 162 consecutive patients with primary lung cancer participated in our study.
The institutional review board approved our study, and informed consent was obtained from all patients regarding the potential risks of both the double dose of contrast medium and two assessments by MRI scanning on a 3.0 T and 1.5 T machine. After the study, 31 patients of this population were diagnosed as having brain metastases. Mean patient age was 61.2 (range, 43 to 80 years). Protocol On the 3.0 T MR scanner (GE Signa VH/i; GE medical system, Milwaukee, USA), the images were acquired using a standard head coil and an actively shielded gradient system with a maximum gradient strength of 43 mT/m. On the 1.5 T MR scanner (Magnetom Vision; Siemens Medical Systems, Erlangen, Germany), a standard head coil and a maximum gradient strength of 25 mT/m were used. All patients were examined after administrating a contrast agent with a double dose of Gd-DTPA (0.2 mmol/kg). First, examinations were performed on a 3.0 T MR scanner and then were subsequently performed on a 1.5 T MR scanner without additional contrast injection.
The scan interval between the 3.0 T and 1.5 T MR examination was less than 20 minutes. The contrast agent used was Gd-DTPA (Magnevist; Schering AG, Berlin, Germany). In all patients, the double dose of Gd-DTPA at 0.2 mmol/kg was administered intravenously as a bolus and scanning commenced immediately. MR imaging included the following sequences on both scanners:
At 3.0 T MRI, an axial 3D SPGR, which is usually used at present, was used (TR/TE/TI = 5.7/1.44/400 milliseconds; flip angle 20°; 2 mm slice thickness; FOV of 220 mm; matrix size of 512×512 ZIP; spatial resolution of 0.43×0.43×2 mm; two acquisition) with a scan time of 3 minutes 30 seconds. At 1.5 T MRI, an axial T1-weighted spin echo sequence was used (TR/RE = 600/14 milliseconds; flip angle 90°; 5 mm slice thickness; FOV of 210 mm; matrix size of 174×256; spatial resolution of 1.2×0.82×5 mm; two acquisition) with a scan time of 5 minutes 30 seconds.
Three radiologists performed randomized, independent blinded review. The three readers were merely informed that all of the patients had lung malignancies. The postcontrast MR examinations of the brain on all of the patients were evaluated. The readers did not have access to other image sets within each study. The presence, size, and number of metastatic nodules were assessed. The postcontrast images were divided into the following two groups: 3.0 T MRI with a double dose of Gd-DTPA and 1.5 T MRI with a double dose of Gd-DTPA. The readers were asked to document the number of nodules. Each nodule in each study was numbered and classified according to its largest diameter measurement: ≤3 mm, 3 mm to 5 mm, or >5 mm. Woo-Suk Chung et al – 102 – Subsequently, if there was any debate about nodule classification, a final interpretation using imaging studies was done until consensus among the readers was accomplished. If disagreements persisted, 3-6 months of follow-up MR scans were obtained for further validation.
For the patients who had follow-up MR scans, these scans were considered positive for metastases if there was a response to the treatment or if there was a growth of nodules identified during the follow-up period. In addition, the sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of the 3.0 T and 1.5 T MRI were calculated using the results from the final interpretation according to size. A quantitative image assessment was performed next. The same lesions on scans of the two different MRI systems were determined by comparing peripheral structures. Signal intensities of adjacent tissue and nodule were assessed by region of interest (ROI) measurements placed identically on both series of images using the same sized circular ROI from the software available on both scanners. Nodule-to[1]adjacent tissue contrast (SI ratio) is defined by SI ratio = ×100 Stissue1 taken as the signal intensity of an ROI assessed over a nodule and Stissue2 taken as the signal intensity assessed over the contralateral white matter.
The signal intensity of a nodule was measured within an enhanced area. In inhomogeneously enhanced nodules, the area of maximum uptake was chosen for measurement. Statistical Analysis The paired Wilcoxon’s signed ranks test was used to compare qualitative scores, and the matched-pair-t test was used to compare nodule SI ratios between the 3.0 T and 1.5 T MRI with a double dose of Gd-DTPA. For all tests, significance was set at p < 0.05, and SPSS software (SPSS Inc. Chicago, US) was used for statistical analyses. Results In the final review made by consensus of three radiologists (Table 1), a total of 143 metastatic nodules were detected by the 3.0 T MRI with a double dose of Gd-DTPA. Of these nodules, 49 nodules were ≤ 3 mm in diameter, 37 nodules were 3 mm to 5 mm, and 57 nodules were >5 mm. A total of 137 metastatic nodules were detected by the 1.5 T MRI with a double dose of Gd-DTPA in the final interpretation. Of these nodules, 43 nodules were ≤ 3 mm in diameter. The 3.0 T MRI with a double dose of Gd-DTPA was significantly more effective at detecting nodules smaller than 3 mm (p = 0.014) than the 1.5 T MRI. However, we found no significant difference in the detection of nodules larger than 3 mm (p > 0.05) (Table 1). In 6 of the 31 cases, six nodules, which were only detected by the 3.0 T MRI with a double dose of Gd[1]DTPA, and missed by the 1.5 T MRI with a double dose of Gd-DTPA, were unanimously agreed upon by all participants in the final interpretation. In three of the six nodules, a growing nodule was detected during a follow-up MR scan which confirmed the presence of metastases (Fig. 1). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of Gd-DTPA due to artifact (Fig. 2). Finally the 3.0 T MRI with a double dose of Gd-DTPA was Stissue1 – Stissue2 Stissue2 Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA – 103 – Table 1. Total Number of Brain Metastases Classified by Size and Detected at the Final Interpretation Size 3.0 T MRI with 1.5 T MRI with p value Gd-DTPA Gd-DPTA ≤ 3 mm 49 43 0.014 3 mm<-≤5 mm 37 37 > 0.05 5 mm< 57 57 > 0.05 Total 143 137 0.014 Note : Data are the number of nodules Table 2. The Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRIs with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm Present Absent Present Absent 3.0 T MRI with Positive 143 00* 49 0* Gd-DTPA Negatiive 000 00* 00 0* 1.5 T MRI with Positive 137 18* 43 18* Gd-DTPA Negative 006 00* 06 0* * Pseudolesions that were detected as nodules by the 1.5 T MRI were detected as vascular structures by the 3.0 T MRI. useful for confirming the presence of these nodules. Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter or better delineation than by the 1.5 T MRI with a double dose of Gd-DTPA. Out of 137 nodules, 65 were brighter (Fig. 3) and out of 137 nodules, 63 were better delineated (Fig. 4). Forty[1]five of 137 nodules were satisfactory in both conditions. By consensus, the final review stated, nodules detected by the 3.0 T and 1.5 T MRI were considered positive for metastases (Table 2). Additionally, there were 18 pseudolesions which were detected as nodules by the 1.5 T MRI, but as vascular structures by the 3.0 T MRI (Fig. 5). The sensitivity, positive predictive values, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 95.8%, 88.3%, and 85.1% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of the 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and Woo-Suk Chung et al – 104 – a b Fig. 2.
A 73-year-old male with multiple brain metastases. Metastatic nodule (a) by a 3.0 T MR image with a double dose of Gd-DTPA show a metastatic nodule (arrow). But (b) the 1.5 T MR image with a double dose of Gd-DTPA cannot show the metastatic nodule by artifact. abc Fig. 1. A 65-year-old male with single brain metastasis. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a small metastatic nodule (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA cannot show the nodule. In (c), a growing nodule was detected during the follow-up MRI with a double dose of Gd-DTPA which confirmed the presence of metastasis (arrow). 100% respectively. For metastatic nodules smaller than 3 mm, the sensitivity, positive predictive value, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 87.8%, 70.5%, and 64.2% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and 100% respectively (Table 3). For quantitative image assessment, the SI ratio in the post contrast sequences (Table 4) was significantly higher in the 3.0 T MRI with a double dose of Gd[1]DTPA than in the 1.5 T MRI with a double dose of Gd[1]DTPA (p = 0.025). Discussion Detection of metastatic nodules is dependent on both their size and contrast ratio (2). As methods to increase the contrast, a higher dose of Gd-DTPA, a higher field strength, and delayed study can all be used to aid detection (2-5, 8-17). Nodules larger than 10 mm are easily detected because vasogenic edema is customarily associated with larger metastases (2). So, when a higher dose of Gd-DTPA is used, the detection rate of larger nodules is not influenced. However, a higher dose is helpful for detecting small nodules because it increases nodule enhancement, yet this method has the disadvantages of increasing the false positive rate and promoting side effects (2-5, 8-14).
A delayed study can also increase the contrast (2). It has been recommended that image acquisition be delayed from 5 to 35 minutes after the administration of contrast material at a dose of 0.1 mmol/kg to ensure optimal detection (2, 15). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of Gd[1]DTPA due to partial volume artifact. Eighteen lesions were detected in the 1.5 T MRI with a double dose of Gd-DTPA, which proved to be vascular structures in 3.0 T MRI with a double dose of Gd- DTPA. The true nature of these lesions was revealed because of the greater morphologic detail visualized by the high field Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA – 105 – a b Fig. 3. A 65-year-old male with multiple brain metastases. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhancement (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhance[1]ment (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter than when observed by the 1.5 T MRI with a double dose of Gd[1]DTPA. Table 3. Estimation of the Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRI with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm 3.0 T 1.5T 3.0 T 1.5T Sensitivity 100 95.8 100 87.8 Specificity – 0 – 0 Positive predictive value 100 88.3 100 70.5 Negative predictive value – 0 – 0 Diagnostic accuracy 100 85.1 100 64.2 Table 4. Results of a quantitative assessment of nodules that were detected by the 3.0 T and 1.5 T MRIs with Gd-DTPA (n=137) 3.0 T 1.5 T P value Nodules-to-adjacent tissue: SI ratio 94.59 63.86 0.025 strength MR image, thus allowing differentiation between true enhancing lesions and sulcal vessels. In our study, each nodules was classified according to its largest diameter as being ≤ 3 mm, 3 mm to 5 mm, and >5 mm because the slice thickness of the 3.0 T MRI was 2.0 mm and 5 mm for the 1.5 T MRI. Therefore this study classified small metastatic nodules as being smaller than 3 mm. Although our study supports the use of a higher field strength MRI with a double dose of Gd-DTPA for increased metastatic nodule detection and for improved nodule enhancement and delineation, the results should be interpretated with caution.
The reason for this is that for patients with two or more brain metastases, additional metastases found with the 3.0 T MRI seem to be of limited clinical importance. The presence of two or more small nodules generally will not change the way the patient is managed. Therefore, it is of utmost importance to identify the difference between none, one, and more than one metastatic nodule.
Patients with a single metastatic nodule located in a respectable region can be treated surgically, and the tumor staged as M1, not M0. However, patients with two or more metastatic nodules are usually Woo-Suk Chung et al – 106 – a b Fig. 5. A 67-year-old female with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows vascular structure (arrow). (b) The 1.5 T MRI with a double dose of Gd[1]DTPA shows a nodular lesion (arrow). A pseudolesion that was detected as a nodule by the 1.5 T MRI with a double dose of Gd[1]DTPA but as a vascular structure by the 3.0 T MRI with a double dose of Gd-DTPA is showed in this figure. a b Fig. 4. A 64-year-old male with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows a metastatic nodule with ring enhancement (arrow). (b) The 1.5 T MRI with Gd-DTPA show a metastatic nodule with ring enhancement (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were better delineated than when observed by the 1.5 T MRI with a double dose of Gd[1]DTPA. treated with radiation therapy and/or systemic chemotherapy (3, 18-22). On the other hand, the use of a higher strength field MRI was found to be helpful in confirming the appearance of an equivocal metastatic nodule. The 3.0 T MRI with a double dose of Gd-DTPA was also useful for the detection of additional metastases in patients with a known lesion detected by the 1.5 T MRI with a double dose of Gd[1]DTPA. Because this also has influence on the sensitivity, positive predictive value, and diagnostic accuracy the 3.0 T MRI with a double dose of Gd[1]DTPA was found to have better results than the 1.5 T MRI with a double dose of Gd-DTPA in our study. Therefore we recommend the use of the 3.0 T MRI with a double dose of Gd-DTPA in only three circumstances: when the findings by the 1.5 T MRI with Gd-DTPA are equivocal, when one potentially surgically respectable nodule is identified, or for detecting early and/or small metastases
There were two limitations in this study. The first limitation was a difference in protocol sequence. The T1 weighted spin-echo protocol was used for the 1.5 T MRI and SPGR technique protocol for the 3.0 T MRI. Detectability of metastatic nodules is more effective with 3.0 T MRI with T1 SE than with a 1.5 T MRI with SE (2). SPGR with thin slice thickness is superior to the T1 spin echo sequence with thick slice thickness due to a partial volume effect. Additionally, SE is not optimum for a 3.0 T due to longer T1- and shorter T2- relaxation times of water protons, which decrease the contrast ratio in the 3.0 T images.17 The purpose of this study was to detect early small brain metastases, so using the SPGR sequence with a 3.0 T MRI, which is usually used at present, has advantages for detecting early small brain metastases. The second limitation was that the scan interval between the 1.5 T and 3.0 T MRI was less than 20 minutes. However, a delayed study increases contrast as mentioned above. The current study found that the SI ratio was significantly higher in the 3.0T images than in the 1.5 T images. Considering the delayed study by the 1.5 T MRI, this limitation emphasizes the better detection rate of the 3.0 T MRI with a double dose of Gd-DTPA. And due to these confounding variables, blinded reviews were performed by three readers. The detectability of metastatic nodules smaller than 3mm was better using a 3.0 T MRI with SPGR than a 1.5 T MRI with T1 SE. Therefore we recommend a 3.0 T MRI with SPGR and a double dose of Gd-DTPA for detecting early and/or small metastatic nodules, furthermore influencing treatment. References 1.Lassman AB, DeAngelis LM. Brain metastases. Neurol Clin. 2003; 21:1-23, vii, Review 2.Ba-Ssalamah A, Nobauer-Huhmann IM, Pinker K, et al. Effect of contrast dose and field strength in the magnetic resonance detection of brain metastases. Invest Radiol 2003; 38: 415-422 3.Sze G, Johnson C, Kawamura Y, et al. Comparison of single[1]and triple-dose contrast material in the MR screening of brain metastases. AJNR Am J Neuroradiol 1998; 19:821-828 4.Runge VM, Kirsch JE, Burke VJ, et al. High-dose Gadoteridol in MR imaging of intracranial neoplasm. J Magn Reson Imaging 1992; 2:9-18 5.Yuh WT, Engelken JD, Muhonen MG, Mayr NA, Fisher DJ, Ehrhardt JC. Experience with high-dose gadolinium MR imaging in the evaluation of brain metastases. AJNR Am J Neuroradiol 1992; 13:335-345 6.Brekenfeld C, Foert E, Hundt W, Kenn W, Lodeann KP, Gehl HB. Enhancement of cerebral diseases: How much contrast agent is enough? Comparison of 0.1, 0.2, and 0.3 mmol/kg Gadoteridol at 0.2 T with 0.1 mmol/kg Gadoteridol at 1.5 T. Invest Radiol 2001; 36:266-275 7.Yuh WT, Tali ET, Nguyen HD, Simonson TM, Mayr NA, Fisher DJ. The effect of contrast dose, imaging time, and lesion size in the MR detection of intracerebral metastasis. AJNR Am J Neuroradiol 1998; 16:373-380 8.Van Dijk P, Sijens PE, Schmitz PI, Oudkerk M. Gd-enhanced MR imaging of brain metastases: contrast as a function of dose and lesion size. Magn Reson Imaging 1997; 15:535-541 9.Yuh WT, Fisher DJ, Engelken JD, et al. MR evaluation of CNS tumors: dose comparison study with gadopentetate dimeglumine and gadoteridol. Radiology 1991; 180:485-491 10.Healy ME, Hasselink JR, Press GA, Middleton MS. Increased detection of intracranial metastases with intravenous Gd[1]DTPA. Radiology 1987; 165:619-624 11.Akeson P, Vikhoff B, Stahlberg F, Holtas S. Brain lesion contrast in MR imaging: dependence of field strength and concentration of gadodiamide injection in patients and phantoms. Acta Radiol 1977; 38:14-18 12.Runge VM. A review of contrast media research in 1999 – 2000. Invest Radiol 2001; 36:123-130 13.Yuh WT, Parker JR Carvlin MJ. Indication related dosing for magnetic resonance contrast media. Eur Radiol 1977; 7(suppl 5):S269-S275 14.Rinck PA, Muller RN. Field strength and dose dependence of contrast enhancement by Gadolinium-based MR contrast agents. Eur Radiol 1999; 9:998-1004 15.Schorner W, Laniado M, Niendorf HP, Schubert C, Felix R. Time-dependent changes in image contrast in brain tumors after gadolinium-DTPA. AJNR Am J Neuroradiol 1986; Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA – 107 – 7:1013-1020 16.Chang KH, Ra DG, Han MH, Cha SH, Kim HD, Han MC. Contrast enhancement of brain tumors at different MR field strengths: comparison of 0.5 T and 2.0 T. AJNR Am J Neuroradiol 1994; 15:1413-1419 17.Nobauer-Huhmann IM, Ba-Ssalamah A, Mlynarik V, et al. Magnetic resonance imaging contrast enhancement of brain tumors at 3 tesla versus 1.5 tesla. Invest Radiol 2002; 37:114- 119 18.Galicich JH, Sundaresan N, Thaler HT. Surgical treatment of single brain metastasis: evaluation of results by computerized tomography scanning. J Neurosurg 1980; 53:63-67 19.Runge VM, Carollo BR, Wolf CR, Nelson KL, Gelblum DY. Gd-DTPA: A review of clinical indications in central nervous system magnetic resonance imaging. Radiographics 1989; 9:929-958 20.Earnest F 4th, Ryu JH, Miller GM, et al. Suspected non-small cell lung cancer: Incidence of occult brain and skeletal metastases and effectiveness of imaging for detection-Pilot study. Radiology 1999; 211:137-145 21.Koutras AK, Marangos M, Kourelis T, et al. Surgical management of cerebral metastases from non-small cell lung cancer. Tumori 2003; 89:292-297 22.Soffietti R, Ruda R, Mutani R. Management of brain metastases. J Neurol 2002; 249:1357-1369. Review Woo-Suk Chung et al – 108 – 통신저자 : 정태섭, 서울특별시 강남구 도곡동 146-92 연세대학교 영동세브란스병원 영상의학과 Tel. 82-2019-3514 Fax. 82-3462-5472 E-mail: tschung@yumc.yonsei.ac.kr 뇌전이종양의발견에있어서Doble dose Gd-DTPA를이용한 3 T MRI와1.5 T MRI간의비교연구 1 연세대학교 영동세브란스병원 영상의학과 2 연세대학교 영동세브란스병원 호흡기내과 정우석1 ·정태섭1 ·김형중2 ·안철민2 ·이재훈1 ·허 진1 ·조응혁1 목적: 작은 뇌전이 종양의 조기 발견은 중요하다. 이 연구의 목적은 1.5 T MRI와 3.0 T MRI 간의 크기에 따른 뇌 전이 종양의 발견율을 비교하는 것이다. 대상 및 방법: 폐암으로 진단 받은 162명의 환자를 대상으로 TNM 병기를 위해 뇌 MRI를 시행하였다. Gd-DTPA 를 2배 용량으로 투여 후, 3.0 T MRI에서 훼손경사회복획득으로 촬영하였으며 그 후 1.5 T MRI에서 T1 스핀 에 코로 촬영하였다. 3명의 방사선과 전문의가 합의하여 MRI를 판독하였으며 정성 평가를 시행하였다. 3.0 T와 1.5 T MRI에서 크기에 따라 민감도, 양성 예측률, 정확도를 평가하였다. 신호 강도를 사용하여 전이 종양과 인접 조직간 의 신호강도 비를 계산하였다. 결과: 162명의 환자 중 31명에서 1.5 T 또는 3.0 T MR에 뇌전이 종양이 발견되었다. 3.0 T MRI에서 143개의 종 양이 발견되었으나 1.5 T MRI에서 137개의 종양이 발견되었다. 6개의 종양이 3.0 T MRI에서만 발견되었으며 크 기는 모두 3 mm 미만이었다. 3.0 T MRI의 민감도, 양성 예측률, 정확도는 각각 100%, 100%, 100%이며, 1.5 T MRI에서는 각각 95.8%, 88.3%, 85.1% 이다. SI ratio는 1.5 T MRI보다 3.0 T MRI에서 유의하게 높았다 (p=0.025). 결론: Double dose Gd-DTPA를 이용한 3.0 T MRI는 3 mm미만의 뇌전이 종양을 발견하는데 있어서 1.5 T
My blog on this subject is attached above, featured recently.
As regards the CQC’s SOAD that Ms Munro refers – as she cannot answer that question I will answer it myself. Never has a CQC SOAD looked into matters properly and even at times agreed with the Trust and Care Home when concerns are raised. They allowed the prescribing of Risperidone, prescribed at Reservoir House Supported Living despite allergy to this drug clearly pointed out to them. They allowed inaccurate prescribing ie 1.75 mg Risperidone which no-one, not even me could cut properly. They have allowed drugging of Elizabeth to enormous quantities whilst at Elysium which clearly did not work. They have ignored the fact she is “treatment resistant” which means poor/non metaboliser and not one of them recommended MRI scans or pathological tests to check for underlying causes when it was obvious none of the drugs worked. I do not feel they even bother to properly look at past file records. Most recently they have ignored the fact that LPFT do not use PANSS recommended by RCPSYCH. Most recently they have ignored or were uninformed that Elizabeth had private scans done which were NOT normal and need further verification OR, if they saw the recent scans done under Lincolnshire United Hospitals Trust they do not have a Tesler 3 which makes my private scans highly accurate. This puts everything in question because of the frequent episodes, stated to be partly blamed on myself.
No, I repeated that Elizabeth feels she is being abused and said this many times during supervised visits. These are Elizabeth’s words, not mine, but how can I disagree when she is being treated differently from everyone else and more like a restricted prisoner.
As for ward round meetings, I am supposedly allocated a 10 minute slot, whereas I should be invited to the whole of the ward round. Quite often I have sat there in front of the computer to no avail and no-one has let me into the Teams meeting or advised that this has been cancelled. I have been studying on a course for some weeks and so have not been able to attend lately but it is clear nothing has changed re the restrictions despite the comments of Ms Munro in her letter.
Yes I did state that the taking away of the mobile phone the family pay a contract on is a breach of Elizabeth’s human rights and ours – the family. The phone contract with Vodafone is only £13.61 pm but it is only right that LPFT should refund every penny whilst they continue to place the mobile into Elizabeth’s locker making it impossible at times for family to get through or for Elizabeth to enjoy listening to music or seeing the comforting pictures of her cat. This whole thing was done before under Dr Shahpasandy under Ash Villa run by LPFT. This carried on for weeks on end and no-one could get through on the phone. It most certainly is an infringement of everyone’s human rights and restrictions are very clearly still in place re supervision, no leave granted and only restricted visitors which does not allow for any quality time after all this length of time. At Ash Villa Elizabeth kept calling the Police in desperation. Don’t know if she has tried to do that here on Castle Ward but this punishment is all aimed at me. It is definitely punishment as I see it because the rest of the family/friends are not subject to any restrictions on visits but are still affected re the phone locked away. Because no impact assessment has ever been carried out as per NHS Guidelines this does not only have an impact on me but others in the family that LPFT have not even considered and Elizabeth herself. What has taking away the phone got to do with engagement with staff? From what I understand Elizabeth is asleep most of the day and up at night so it would not be affecting her ability to participate in any ward round meetings or activities on the ward. What treatment plan! They do not use the recommended PANSS. Elizabeth should be given a copy of her care plan. There is clearly no discharge plan of any kind and acute ward detention on a never ending section continues now for over 2.5 years with no end in sight. Now Ms Munro goes on to state the following:
“ELIZABETH’S PHONE ACCESS WAS LIMITED FOR A FIXED PERIOD OF TIME AS PART OF A COMPREHENSIVE CARE PLAN THAT CONSIDERED HER HUMAN RIGHTS. THIS WAS TO ENSURE THE RESPONSE TO HER PHONE USE DID NOT ADVERSELY IMPACT HER ENGAGEMENT PLAN WITH, OR THE EFFICACY OF THE TREATMENT PLAN. THIS WAS CEASED ON MONDAY 5 FEBRUARY 2024 FOLLOWING REVIEW OF ALL THE RELEVANT FACTORS.”
So, first of Elizabeth why is she still without her phone as it is held in her locker so that she cannot access at all times as she does not have the key. The ban (not limitation) has been ongoing for months now and it has been extremely difficult for all of us to contact her even the family members and friends were not put through immediately as a member of staff had to be available to go and unlock her locker and hand the phone to her or else in my case only for two members of staff to sit there listening in to all phone calls which is in breach of Art 8 HRA and the Equality Act 2010. I honestly truly do not know what on earth Ms Munro means by stating “care plan that considered her human rights”. This is absolute rubbish and I believe that not only do LPFT need to implement the Oliver McGowan Training Programme but it is no wonder there is no sign of that if they do not understand what basic human rights are and what is meant by acting ultra vires, relying on Bolam Law when it should be Montgomery – all hiding behind each other as regards decision making. Of course this is a breach of human rights as not having the phone or being readily able to access it whilst held under MHA 1983 and is an abuse of power and process as well as the law. What right do a public authority have to do this and this is NHS care. For a short while Elizabeth was sent to Cygnet Durham. At first she did not have her phone but then this was given back to her as at least Cygnet realised this was in breach of the law unlike the NHS. Under the MHA detention should be the least restrictive care. The most untruthful comment Ms Munro makes is that restrictions ended on 5 February. So what I did was take with me the letter to show Elizabeth. I was told by the two HCAs that I could not just give the letter so I said “why not”? They said they had to show the manager first (I then said Oh I see the Management are involved in all this?) The Manager to Castle Ward is Kashmir Moons. So they took the letter from me. I read the contents of the letter before I gave it to them. I asked that they hand the letter back to Elizabeth and will check she has it when I next have contact. Contact is only if Elizabeth asks for the phone but I get the impression she is asleep a lot during the day and up late at night. This would explain why meals continue to be missed.
Ms Munro then goes on to mention an “incident” on Xmas Day for which internal investigations and review of all relevant evidence was undertaken and following that re-establishing of prior arrangements.
This is NOT GOOD ENOUGH MS MUNRO. For a start there was no incident whatsoever but Elizabeth got upset with the second lady – a HCA told to sit in the small visitor’s room on Xmas Day of all days and write notes. It was the writing of notes that got Elizabeth upset and she reacted. I had also found out that the Clopixol depot had been reduced by 50mg and I was told to leave the ward when a crowd of about 5 staff gathered outside the visitor’s room including men which was very intimidating. When I left the visitor’s room all Elizabeth did was to shout and they grabbed her throwing her into seclusion and injecting her afterwards. Why inject when all someone needs to do is to calm down but they tend to do this after every ‘episode’ that looks like a fit. Why rapidly tranquilise when she has calmed down. Xmas Day was ruined and spoiled and I did not know they called the Police on me. When I found out I opted to complete a S9 statement but I doubt anyone from the Trust did that and they should have been asked to do after all to call Police out for no reason is very bad. All this is being done to intimidate and threaten using Police as a weapon when in fact Elizabeth trusts the Police more than MH professionals and regarded them as “friends”.
So this has justified the banned visits whilst internal investigations took place. Not one apology given in her letter.
Ms Munro goes on to explain about the Neurologist Appointment being unattended but what Ms Munro does not know is that I in fact attended with a copy of the private scans done on a Tesler 3 scanner. I knew about the appointment because Elizabeth told me and shared her letter with me. Again the MH were keen she did not attend by the looks of it. They have done everything to stand in the way of her Neurologist appointments but I met the Consultant Neurologist myself. I knew that scans were done in addition by the Trust in November 2023, Mine were done end of May 2023. What I did not know at the time was that they did not have a Tesler 3 but a 1.5 scanner so it is no wonder their scans are not accurate as opposed to mine. What I am concerned at was their response. The Clinical Lead Emily Scott said they had no knowledge of the Neurologist appointment and this was at 11.00 am so I bet Elizabeth was asleep and no-one got her up for it. Now they propose a further scan in Sheffield because they do not have the latest scanner when I have produced scans done privately under a Tesler 3. “This aspect of Elizabeth’s healthcare is ongoing”. Good – glad to hear it since all this should have been done upon arrival but the team were too busy trying to take away my role as POA and NR to consider physical health needs.
Regarding the telephone call where a new staff member had limited English, I only went by what Elizabeth said when I asked to speak to the new member of staff over the telephone. This might have been just an excuse on the other hand.
Concerns on Missing Meals – yes Adults safeguarding were supposed to look into this and the ward is supposed to keep daily food and fluid chart to document intake. At Ash Villa this was a frequent occurrence but I still think missing meals goes on as if Elizabeth is frequently rapidly injected then she is asleep during the day or cannot get up for meals and misses them and in the evening there is just a sandwich. I am not saying this is happening now on a daily basis like before however it still does occur and again laundry – this is what she was doing herself in her flat without support. This is the level of decline that now Elizabeth needs someone to help shower her, do her washing etc etc whereas before she was doing this herself and even using a bank card, going shopping, using buses whilst in her independent flat. Substantial decline because of her treatment worse than a restricted prisoner. These comments again came from Elizabeth who said she had run out of clothes but staff do not seem to understand autism. There is no sign of the Oliver McGowan Training and the other day when we visited she told me that Dr Khokhar said “you have not got autism” – I pointed out to the two staff supervising that autism was what Elizabeth had researched as her condition and should be respected – after all there is no end of evidence and every screening came out positive by other institutions and other doctors. I, on the other hand think there is brain injury which may have been present before under Enfield and covered up as it says on the discharge note “abnormal findings on scan pointing to cns”. Since then there have been 10 doctors (psychiatrists) keen to treat as a MH patient and ignore the discharge note and private scans up until the frequent life threatening episodes which resulted in A&E to the point this could no longer be ignored.
“We aim to provide high quality care and treatment to all those we support and are sorry you have had to escalate your concerns. We value opinions of those who use our service as it gives us vital insight into any care we provide and informs us when improvements are necessary. We thank you for raising these concerns.”
Taking the above into consideration here are the improvements:
Stop taking the phone away and using this and restricted visits and cutting of leave as an excuse unless someone fits the criteria of s11:15 MHA Code of Conduct. Elizabeth is an Adult and should not be treated this way and also you are in breach of Art 8, Art 5, Equality Act 2010 plus Art 3.
You should settle up with the phone bill and thinking about it the private scans that were accurate unlike those done under a 1.5 scanner.
You should allow leave/visiting rights to resume unrestricted and give the phone back to Elizabeth to keep in her handbag like everyone else.
You have discriminated against us as a family, not just Elizabeth that has impacted against even those not being punished ie other members of family.
Elizabeth misses her cat and wishes to come home to visit and to live. You have been looking at care homes in W Sussex and Yorkshire without any thought to rest of family.
I have had serious verbal threats of indefinite banning of visits at a Ward Round in December because of flawed allegations of some kind of incident when nothing happened except for police time to be wasted.
I have presented you with an invoice and would appreciate prompt settlement. I shall do either an additional or amended invoice to include the private highly accurate scans seeing as they were needed in the first place. It is therefore only fair that the Trust pays.
There is no sign of the Oliver McGowan Training? Where is this training?
There is no sign of proper diagnostic tool PANSS and why not when recommended by RcPsych?
The way you have handled everything has been a disgrace. To try to take away the POA. You failed at this.
To try to displace me you used County Court and did so in secret. Secret courts should be banned. This is of public interest as it is public money. The law needs to be tightened so that there is more accountability which could save vast amounts of public money at County Courts where Judges do not have the remit to properly look into matters.
To present papers and to keep getting HCAs to report negatively against me is bullying and I am entitled to see everything written against me.
It is wrong to treat me differently to rest of family and I should say this is clearly discrimination.
The ward is very noisy and this affects Elizabeth along with the very highly bright lighting.
The CQC should look into the legality of the Section 3. It is more like a Section 37/41. What right do you have to hold Elizabeth like this and treat her like a vegetable when each and every one of the capacity assessments are flawed. I should know as I have done the course. She was not even on a section in the former area so how do you explain this?
As for the MHA this needs urgent amended because Trusts and Councils like Lincolnshire and Enfield/Barnet Enfield and Haringey MH Trust have found a way to twist the law to their own ends and use social services against you and they abuse the MCA which I have studied thoroughly in order to take away a vulnerable patient’s autonomy when they have got capacity.
I now want all the files from both records and everything written about me so that I can correct everything which might take me years and years to do. How can you give decent care if your records are untruthful and inaccurate.
I have now highlighted the need for a new scanner in two areas – Lincolnshire and Weston. This is essential to ensure proper diagaosis.
The last thing I am going to point out is about Capita doing the assessments for PIP. I explained that Elizabeth was still in hospital, not in receipt of PIP and declining. If a vulnerable person got a call like this it would be extremely upsetting. I now have an appointment for an assessment coming up shortly.
It is important for anyone having an MRI scan to check which scanner their Trust has as I have wondered why the scans at Lincoln County Hospital have not shown up the same details as the scans I had done privately and now I know why. I have found out that they use a 1.5 Tesla scanner.
I immediately contacted my MP, Victoria Atkins to advise that Lincoln United Hospital Trust should be provided with the most accurate scanner which to my knowledge is the Tesla 3.
I am just warning everyone to check and question in order to ensure they receive highly accurate scans.
I have found out that the following:
Diagnostic imaging department at The Lincoln Hospital, Lincolnshire offers a wide range of diagnostic tests and imaging examinations.
All imaging is processed using electronic technology known as CR (Computed Radiography) and PACS (Picture Archiving and Communication System) which enables fast, electronic display of all images and reports.
At The Lincoln Hospital diagnostic imaging equipment is used that includes a wide bore 1.5T MRI scanner, ultrasound and a mobile 64-slice CT scanner (available every other Tuesday).
The diagnostic imaging department at The Lincoln Hospital offers the full range of routine and specialist services including:
The main difference between a 1.5 Tesla (T) MRI scanner and a 3 Tesla MRI scanner lies in their magnetic field strength.
1.5 Tesla MRI scanners have a magnetic field strength of 1.5 Tesla, while 3 Tesla MRI scanners have a magnetic field strength of 3 Tesla.
Here are some implications of this difference:
1. Image Quality: Generally, higher magnetic field strength (such as 3 Tesla) can provide better image quality compared to lower field strengths like 1.5 Tesla. This higher field strength can lead to increased signal-to-noise ratio, which results in clearer and more detailed images.
2. Resolution: With higher magnetic field strength, there’s potential for higher spatial resolution, allowing for more detailed imaging of structures within the body.
3. Scan Time: In some cases, higher field strength MRI scans may require shorter scan times to achieve comparable image quality to lower field strength scans. This can be beneficial for patients who may have difficulty remaining still for long periods.
4. Cost and Availability: Generally, 3 Tesla MRI scanners are more expensive to purchase and maintain compared to 1.5 Tesla scanners. Additionally, they may not be as widely available as 1.5 Tesla scanners in all healthcare facilities.
5. Clinical Applications: Both 1.5 Tesla and 3 Tesla MRI scanners have their own set of clinical applications. 3 Tesla MRI scanners are often preferred for certain types of imaging studies such as neurological imaging (brain and spinal cord), musculoskeletal imaging, and research applications where high-resolution imaging is crucial. However, 1.5 Tesla scanners are still widely used and may be preferred for certain clinical scenarios where higher field strength may not be necessary or may pose additional risks.
In summary, while both 1.5 Tesla and 3 Tesla MRI scanners serve the purpose of imaging internal structures of the body using magnetic resonance, the difference in magnetic field strength results in variations in image quality, resolution, scan time, cost, and clinical applications. The choice between the two depends on factors such as the specific imaging needs of the patient, availability of technology, and clinical judgment.
Surely the needs of the patient is paramount in terms of the provision by every Trust of the Tesla 3 scanner to ensure without doubt that they get the most accurate scans and I have therefore proven that the current 1.5 Tesla scan done by the hospital has missed vital details that need verification and checking out because I had a private Tesla 3 scan done for Elizabeth. I have told my MP that a Tesla 3 scanner is urgently required at Lincolnshire United Hospital Trust.
What makes this letter so untruthful is that the mobile phone is still held in the locker, locked away and only supervised calls and visits are allowed by the truly awful Lincolnshire Partnership Trust rated “GOOD” by the CQC. If restrictions had ended on the 5th February as Ms Ann Munro states then why are they still continuing on the ward in that case or why hasn’t this been relayed to the ward? Dr Waqqas Khokhar and team continue relentlessly with restrictions that are a complete infringement of Human Rights – breach of Art 8 and Equality Act 2010. The restrictions are ONGOING and it was threatened by Elizabeth’s doctor that the ban was indefinite. I have issued LPFT an invoice that is only £50 for the phone contract family pay to Vodafone monthly and the cake I brought for Elizabeth’s Birthday that got put in the bin. It seems like noone is doing anything about anything and all staff acting ultra vires. Yesterday as I have to be seen to be doing everything I can to resolve matters I chased up the investigations I called for under the NMC, GMC, ICO and HCPC – Adults Safeguarding have concluded their investigation but a couple of days ago Elizabeth phoned me and said she had missed meals and only had crisps to eat. This all goes to show that the “care” Elizabeth is receiving is not right or appropriate and that acute wards are totally unsatisfactory to anyone with sensory issues and those who claim or have been diagnosed to have autism, LD so in that case why are so many trapped for years and years on end.
The reason is not because there is nothing in the community but it is all down to funding. We did not ask for anything but had hoped for a better life in a new area. Inevitably the outcome is disablement and then that vulnerable person becomes institutionalised for the rest of their lives and placed under DoLs – another form of imprisonment. Stripped of their capacity, human rights do not apply.
Now there needs to be more done as what the NHS is providing is totally wrong and the way they go about bullying families with litigation lasting months and months in secret courts is totally and utterly wrong.
If Ms Munro claims that the restrictions have ended with the phone then this needs to be sorted out as members of staff were/are oblivious to this. There seems to be lots of bank staff supervising and they use HCAs and they are writing negative notes to build up a picture against me. It is the ultimate bullying. I now take a witness with me because they keep calling out the Police and wasting their time in desperation to portray me as a nasty person but I am being totally honest here revealing the truth and nothing but the truth. There is no way I would be going to these lengths publicly if I was not speaking the truth and from what I see I am not alone with others writing about the shameful care provided under MH in the UK that has no accountability. They have also gone out of their way to stand in the way of pathological tests and referrals to Neurologist which was on 3 January but I was told by the Clinical Lead Emily Scott that they knew nothing about this appointment. Oh yes they did! I attended instead with the private scans done under a Tesler 3 scanner which Lincolnshire do not appear to have and which are highly accurate.
I write to respond to the queries and concerns you shared with the Care Quality Commission (CQC) between 14th November 2023 and 28th December 2023; You said that the SOAD (second opinion appointed doctor) did not take account of Elizabeth’s allergy to a medication. We are unable to answer points related to the decisions made by the SOAD as they come under the remit of the CQC.
You said you are concerned that Elizabeth is being abused. Investigations into Elizabeth’s safety have been initiated and the trust are cooperating with these as requested.
You claimed that on occasions you had not been allowed into the ward round meetings.
The ward confirmed that you have the link to attend a designated slot for the weekly ward round meeting. They have noted occasions where you have not joined the meeting.
You have said that Elizabeth having her mobile phone removed is a breach of her human rights. Elizabeth’s phone access was limited for a fixed period of time as part of a comprehensive care plan that considered Elizabeth’s human rights. This was to ensure the response to her phone use did not adversely impact her engagement with, or the efficacy of, the treatment plan. This was ceased on Monday 5th February 2024 following review of all the relevant factors.
You claim that details recorded of the incident that took place on 25th December 2023 during your visit to Castle Ward are untrue and have resulted in your visiting arrangements being suspended. Visiting arrangements were temporarily suspended while internal investigations and review of all relevant evidence were undertaken and that visiting arrangements have now been re-established, as set out in letter dated 5th February 2024.
You said that Elizabeth was not able to attend the neurology appointment in January 2024. Elizabeth was not able to attend a neurology appointment in January 2024, however following discussions with professionals at United Lincolnshire Hospitals Trust, alternative provision was facilitated so that the relevant clinical staff could attend Castle Ward to see Elizabeth. This was organised to minimise any disruption to Elizabeth and maximise her potential engagement with the process. This aspect of Elizabeth’s healthcare provision is ongoing.
You described a telephone call to the ward where a new staff member had very limited English. Your feedback on this staff interaction has been passed on to the relevant teams to ensure any necessary reviews are undertaken. You expressed concern that Elizabeth was missing meals which was impacting on her behaviour.
The ward is continuing to keep a daily food and fluid chart to document Elizabeth’s intake. This also ensures any additional support can be provided to Elizabeth where appropriate. You said that Elizabeth had lots of washing and that she was not being supported with this. The ward has confirmed that Elizabeth is usually known to attend to her own laundry independently. Patients can access the laundry room at any time in the company of staff and Elizabeth can request support from staff for this purpose. We aim to provide high quality care and treatment to all those we support, and we are sorry that you have had to escalate your concerns.
We value the opinions of those who use our service as it gives us vital insight into any care we provide and informs us when improvements are necessary, and we thank you for raising these concerns.
Thank you for bringing your concerns to our attention. LPFT mental health services strive to deliver the best care to all our service users and their families/carers all the time and I regret this has not been your experience. NHS Complaints Advocacy is also available at every stage of the complaints process.
VoiceAbility can be contacted by calling their Helpline on 0300 303 1660 or via email helpline@voiceability.org If you are not happy with how we have dealt with your complaint and would like to take the matter further, you can contact the Parliamentary and Health Service Ombudsman. The Ombudsman makes final decisions on complaints that have not been resolved by the NHS, Government departments and some other public organisations. Their service is free to everyone. There is a time limit for making your complaint to the Ombudsman so you should do this as soon as possible.
To take a complaint to the Ombudsman, or to find out more about the service, go to https://ombudsman.org.uk/making-complaint or call 0345 015 4033. Yours sincerely, Checked and electronically signed to speed delivery.
Extracts of Letter from Sarah Connery, CEO Trust HQ, St Georges Long Leys Road, Lincoln lN1 1FS
“This is a complex case involving ongoing and intersecting legal and complaints procedures. There have been involvement from multiple organisations in managing this case including Care Quality Commission, Lincolnshire Police, Lincolnshire Integrated Care Board, Lincolnshire County Council’s Safeguarding and Legal Services, LPFT MHA and Legal Services Team in addition to the Patient Experience Team and Safeguarding Team.”
There is no complexity. Elizabeth has somewhere to live and wanted to move in 2021. She was living in a high rise block of flats without support. A meeting was held with the CMHT before moving but treatment not continued through no fault of mine. She was being reduced off it due to discharge note stating “abnormal findings on scan” in any case. Since October 2021 she was taken and imprisoned in 5 institutions with 10 doctors involved. Treated like a restricted prisoner, no leave, restrictions on visitors, phone confiscated and family contact discouraged, this has been “care” under Lincolnshire Partnership Trust to date. Months of investigation by Public Guardian Office following malicious allegations of abuse by various professionals found in our favour. With so many agencies involved you would think that something would have been done about this situation by now and that there would be an end in sight but the abuse continues with no end in sight. There have been months of legal action against me as though I was a criminal at County Court with involvement of Lincolnshire County Council to achieve the goal of displacement of NR only for me to become NR again thereafter to another family member. All along there was mention and threat of placement into care without any respect for my daughter’s wishes or that of her family. The little bungalow remains empty that could have provided happiness to my daughter in the right environment of the small community where I now live close to sea and wildlife reserves and peaceful unlike an acute ward.
Ms Connery mentions my blog and that I wrote 70 emails. I don’t know where she gets that figure from – as if I had time to write so many! During many months of court proceedings against me I received an email from Ms Anita Lewin who held overall responsibility: it was not of best interest to respond to complaints. LPFT have now set up an email address where I am supposed to write to but responses I have received are not related to my complaints which remain unanswered for the most part. I have had one letter after another banning me from visiting without any alternative arrangement in place. Ms Connery refers to “due to concerns from the patient’s MDT made on clinical grounds in line with MHA Code of Practice 2015 shouldn’t that be 1983? paragraph 11:14. So here below is the MHA CODE OF PRACTICE 1983: – only part of 11:14 was mentioned – here is the rest:
Restrictions or Exclusion on Clinical Grounds
11.14
From time to time, a patient’s Responsible Clinician (Dr Waqqas Khokhar) may decide, after assessment and discussion with the MDT, that some visits could be detrimental to the safety or wellbeing of the patient, the visitor, other patients or staff on the ward. In these circumstances, the Responsible Clinician may make special arrangements for the visit, impose reasonable conditions or, if necessary, exclude the visitor. In any of these cases, the reasons for the restriction should be recorded and explained to the patient and the visitor, both orally and in writing (subject to the normal considerations of patient confidentiality). Wherever possible 24 hour notice should be given of this decision. So from this it is in fact the Responsible Clinician’s decision but we have not had proper explanation re risks to others or patient???
Restriction Or Exclusion on Security Grounds
11.15
The behaviour of a particular visitor may be disruptive in the past, to the degree that exclusion from the hospital is necessary as a last resort. Examples of such behaviour include: Incitement to abscondSmuggling of illicit drugs or alcohol into the hospital or unitTransfer of potential weaponsUnacceptable aggressionAttempts by members of the media to gain unauthorised access. None of this applies
11.16
A decision to exclude a visitor on the grounds of their behaviour should be fully documented and explained to the patient orally and inwriting.Where possible and appropriate the reason for the decision should be communicated to the person being excluded (subject to the normal considerations of patient confidentiality and any overriding security concerns.No this has not been done at all. What risks exactly and why to other patients and staff when I am not sitting in the lounge area but small visitors room elsewhere.
I would also point out that nothing was properly explained about the ban and no warning given. Paragraph 11:14 was mentioned but not all of paragraph 11:14. As you can see paragraph 11:14 states about making special provisions and explaining in full. This was not done. All we constantly hear is “it is an MDT decision”. NO! It is the decision of the Responsible Clinician who is Dr Waqqas Khokhar. Everyone else on the ward is dutifully acting upon instructions that are in total breach of the law and their own Code of Conduct. It is astonishing why no one raises a hand to question what is going on as it is clearly detrimental to the patient and not conducive to her recovery. Elizabeth has even got upset by staff sitting there taking constant notes (no doubt writing in not a very nice way) behind my back. This happened on Xmas Day when staff called Police and tried to blame me.
When you ban someone from visiting LPFT were supposed to carry out an Impact Assessment but this was not done. The Impact Assessment should have been carried out on myself and Elizabeth with copy to her sister, NR who was LPFT’s choice to displace me in court last year. No correct procedures were done. Ms Connery mentions about impact “due to continued concerns about Elizabeth’s health and wellbeing and the need to protect the safety and wellbeing of staff and other patients on the ward” . What is she talking about? What is meant exactly about the safety of staff and other patients? What is Ms Connery trying to imply that I am someone who has gone onto the ward with weapons, threatening members of staff when I have been in visitor’s rooms on the occasions when I was allowed to visit. Why was Police time wasted on more than one occasion? why are they using bullying tactics to intimidate me as a visitor? Ms Connery has simply repeated the malicious allegations coming from a person in charge who is reliant on MDT backing and without any substance or evidence. When I visited Elizabeth there are little side visitor’s rooms and CCTV throughout to monitor behaviour of any visitors. So concerned were myself and a visitor that we opted to complete a Police Section 9 statement but Police were not even bothering to investigate a so called incident so ‘serious’ that a member/members of staff called Police on Xmas Day wasting their time. It is totally unjustified to make out I am a risk in any way and to restrict contact getting staff to write nastily behind my back and that is what is upsetting to Elizabeth. Staff constantly writing notes. It is no doubt an abuse of power and process. It is all done with the intention of making you feel intimidated and uncomfortable to go and visit. During my visits, I spent time in the small box room of the visitor’s rooms not socialising with staff or patients on the ward itself. Sometimes one other patient would knock on the door of the visitor’s room Elizabeth introduced me as her friend. This friend knew I always brought food and nice things onto the ward that Elizabeth would share but now all has stopped due to shortage of space in the fridge. It is unjustified of Ms Connery to say these comments and for me to have received an extremely nasty threatening letter alleging intimidation and aggression towards staff at Trust HQ when all I did was sit in a corner writing a note and the only person was a receptionist and the visit was witnessed by a friend. I viewed CCTV footage and there was nothing to see relating to such behaviour as described in their letter.
“The second part of the complaint states: Ms Bevis is of the opinion that Elizabeth’s phone is being withheld indefinitely” To Clarify, Elizabeth’s phone access and use is being managed in line with her care plan to protect her health and wellbeing as part of her mental health treatment.” This has been going on for months now with no end in sight. We pay a Vodafone contact for the phone and it is only fair LPFT refund the money to Elizabeth in the circumstances.
Not having full access to her mobile phone means that Elizabeth can no longer listen to her music, see pictures of her cat readily and all phone contact numbers are in the phone so she cannot make calls to anyone and is encouraged to use their phone on loud speaker in the visitor’s room. This is inflicting upon the rest of the family not just me. It is abusive and inhumane to take away the phone from a vulnerable person held like a prisoner on never-ending sentence. It is degrading and undignified to put members of staff supervising all calls, all visits etc. How would they like it? This is not being done to protect my daughter but to protect themselves.
Ms Connery ends by stating “hope this letter provides reassurance around the care afforded to Elizabeth in regards to the concerns raised.” No it does not and it makes you question all the more how someone in a high up position who is well aware of everything can just sit back and do nothing.
As for care, this is not care it is worse than prison and Elizabeth described this in her own words “HELL ON EARTH”. That is what she thinks of LPFT’s “care”. The response from Maria Caulfield would put these comments into dispute.
LETTER FROM THE RT HON MARIA CAULFIELD MP
I have another letter from the Rt Hon Maria Caulfield MP (Parliamentary Under-Secretary of State for Mental Health and Women’s Health Strategy 39 Victoria Street, London SW1H 0EU. The letter is dated 8 February 2024 to the Rt Hon Victoria Atkins.
“As well as concerns about abuse, Ms Bevis wrote about potential diagnoses for her daughter which might affect her mental health and/or affect her capacity to make specific decisions although I cannot respond about the specifics I have set out some general rules and guidance which I hope Ms Bevis and her daughter may find helpful.”Not quite. They (the MH team) will not budge on “paranoid schizophrenia” yet Elizabeth constantly says she is autistic but there are certainly a lot of questions that need to be answered and it is not unreasonable to question when you have certain evidence to the contrary that needs thorough checking out.
My comments to the above are that with regard to potential diagnoses, pathological tests were denied to my daughter from the moment we arrived in Lincolnshire, whereas in London for the first time ever her physical health was being taken very seriously. I had hoped for continuation of the same level of care into her physical health but sadly that has not been the case. It should have all been quite simple – continuation of what was being done in former area but instead we have encountered nothing but bullying. All physical health appointments eg Neurology cancelled as “unnecessary. The Discharge Note from Enfield mentioned “abnormal findings on scan” . To date I have not been able to find out what was mentioned twice referred to. This was drawn to the attention of the various psychiatrists Elizabeth under LPFT in particular at Ash Villa and Castle Ward but thought unnecessary to explore further pathologically reliant on a scan done back in 2015 stated as being “normal”. This prompted me in a small window of opportunity to have private scans done through S G Radiology in a mobile unit that do not appear to be normal.
“ The Government makes it clear, in the Care Act’s Care and Support Statutory Guidance, Local Authorities must ensure that the services they commission are safe, effective and of high quality. Where anyone alleges poor care, neglect or abuse we expect those providing the service, local authorities and the Care Quality Commission (CQC) to take swift action. “
Unfortunately, sadly this has never been the case which is why we moved from Enfield. Once you complain this is where you see the ugly side of those supposed to care whether it be Trust or Council .Because care provision was non existent in former area and various supported living/housing and care home were appalling that is why I tried to provide a decent home for Elizabeth in the right environment which has backfired on me.
Unfortunately in all this time the CQC have done nothing to stop the abuse in law/human rights and allowed continuation to date. Letters I have received from two CQC inspectors are not emphatic and you never get to hear what if anything is being done about the situation. One inspector described the CQC as a “business”. When other patients step in to do the safeguarding as at Ash Villa something is very wrong and there is no accountability. What is the point of these organisations meant to protect vulnerable people when nothing appears to have been done. They most certainly do not take swift action and have allowed the situation to continue.
One again I am hearing “if Ms Bevis is not satisfied with the way a provider or LA has dealt with a complaint she can escalate it to the Local Government and Social Care Ombudsman : I have done all that! I had to even dispute their response which allowed for slight amendment but nothing done whatsoever. he LG Ombudsman only wanted to investigate what happened prior to moving and that was not looked at properly. We had Judicial Review Solicitors appointed yet nothing was mentioned. Another Joint Party Investigator was supposed to look at what happened once we had moved but this adviser refused stating it was purely a Health matter only for PHSO. Then the PHSO refused as they were waiting for everything in writing from the Joint Party Ombudsman. In the end I simply copied their email to the PHSO but still they did not get involve. Both cases were simply shut down without any proper investigation. My dealings with Professional Bodies have all appeared the same in that they are not there to safeguard the public but their own members and the “Professional Standards Authority” do not have powers to intervene.
“If Ms Bevis has not already done so she may also wish to seek independent legal advice and consider contacting the Citizens Advice Bureau which can provide help on a case-by-case basis.” This is not helpful as they cannot help in what is clearly issues of human rights. As for getting legal advice this is impossible – you are simply met with the same response constantly that they have “no capacity”.
Ms Caulfield also comments: “the Mental Capacity Act 2005 (MCA) is designed to protect and empower people who lack the mental capacity to make a decision themselves, which may include people with advanced dementia, autism, learning disabilities and acquired brain injury. The Deprivation of Liberty Safeguards DoLs which form a key part of the Mental Capacity Act can be used to authorise the person being accommodated in a hospital or care home in circumstances the amount to a deprivation of liberty for the purpose of providing care or treatment.”
Here is my response: No it does not protect.
If Elizabeth lacks capacity, as suggested their duty of care/standard of care in medical negligence is at a higher level. Why is she being neglected on the ward to the extent that no one is even checking that she is being properly nourished? The LPFT and LCC are abusing the capacity assessment process to restrict or deny Elizabeth’s fundamental rights to patient autonomy to facilitate their own interests or convenience. This includes denying her rights to privacy and a family life by subjecting her to oppressive supervised visits. The LPFT are abusing their powers under the Mental Health Act 1983 to deny Elizabeth and her family fundamental human rights, not in order to prevent or control risk or to achieve the objectives of section 2 of that Act but simply to benefit themselves and to obtain control to abrogate their actual responsibilities.
The MHA 1983 was designed to protect the interest of the mentally ill, not provide a convenient set of excuses for clinicians, nurses and social workers.
Unfortunately, Neither the MCA 2005 or the MHA 1983 is protecting the most vulnerable people at all. The very people who should be caring towards my daughter are being abusive and denying my daughter and that of others the right to see their families unrestricted. I suppose they go along with their orders by Responsible Clinicians because as I have experienced there is a culture of bullying within the NHS so no one dares speak out.
Ms Caulfield further states:
“Any restrictions placed on a person must be in that individual’s best interests and necessary and proportionate. Consideration should also be given as to whether less restrictive options could be used. An overview of the MCA and how it is applied can be found here: www.scie.org.uk/mca.”
I have just completed a wonderful course through SCIE on mental capacity and “best interests” so I know very well that nothing LPFT are doing is in the slightest bit correct.
Re: displacement of NR previously covered, this shows overwhelmingly the need to update the MHA, our case makes a mockery of the MHA and extortionate costs of litigation through presentation of untruthful reports and comments put before court. This is why courts should be open and transparent. I could write a book on it!. The MHA is not fit for purpose and the MCA is also failing those who are vulnerable and their families.
Ms Caulfield mentions about my complaint of restricted visits and contact, In my case banning: “contact with family and friends is a crucial part of a person’s care and no one should be denied reasonable access to visitors whilst they are a resident in a care home or a patient in a hospital or hospice” “This includes having a loved one at a hospital bedside for a crucial diagnosis discussion, receiving assistance from a “care supporter” or simply going for a walk with a family member or friend. The statutory instrument (SI) on visiting (www.legislation,gov.uk/uksi/2023/1402/introduction/made laid on 18 December 2023 inserts a new fundamental standard on visiting and accompanying to the CQC regulations. This will commenceon 6 April 2024. Try telling that to LPFT, a law unto themselves.
About Elizabeth being sent to Durham, Ms Caulfield writes:“inappropriate out of area placements (OAPs) occur when people are admitted to a mental health inpatient ward outside of their local area due to lack of available beds locally. We remain committed to eliminating all inappropriate acute out of area placements for adults (people age 18 and over). NHS England continues to work with the worst performing areas supporting them to improve, and we are working with them to ensure that systems prioritise this, including a focus on discharge and flow. To support adult social care and discharge up to £2.28 billion has bee made available in 2023/2024 and £4.7 billion in 2024/25. This can be used to support discharge from mental health inpatient settings, reducing bed occupancy and OAPs.
I hope this reply is helpful.
I would have liked action rather than words and intervention because there is no end in sight of the never-ending detention and abuse of my daughter; assessments have gone on behind out backs for a care home in West Sussex so very far away from all the family. I am not alone and all of this is being done because I as mother has dared to question certain private scan results and my next blog will be all about that.
These are Elizabeth’s wishes:
FRIDAY 10TH NOVEMBER 2023
“MY IDEA” BY ELIZABETH BEVIS
“I WANT TO EVENTUALLY COME HOME TO LIVE WITH MY MUM IN THE ANNEX THROUGH COURT OF PROTECTION. I MISS MY MUM GREATLY AND WANT TO GO HOME TO HER”
There is no way she would have written this if I was the person who a team of circa 30 try to make look bad and what on earth have they been writing behind my back to justify this and call Police out several times for no reason. To think a team of 30 meet regularly and discuss you behind your back and then make the decision to stop contact because of concerns they do not make clear or is it really the team, rather than the person with overall control of the ward ie the RC. Nothing is being done to protect the public or the vulnerable person from such abuse. By going along with what is ordered by certain people at the top staff are acting ultra vires and breaking the law as well as their own Codes of Conduct. They get away with it because their own professional bodies do nothing to intervene and because the Professional Standards Authority have no power to intervene. Also this whole situation would not be still ongoing if it were not for those at the very top of the Trust who choose to support rather than intervene the actions of certain professionals and allow the law to be broken.
Not everyone has access to a computer or internet but I am totally inspired by my contact who is 91 having to stand up for her son who by the sounds of it has been totally misdiagnosed and denied the correct pathological tests by the NHS.
A Carer’s Story by “A” (I am using the exact words of my guest blogger as written in a letter by request)
“I have been involved with Mental health for many years as a carer for my son, even though the diagnosis is totally wrong.
My son has had nothing but persecution – stress – no life whatsoever.
Resistant to some medications.
The service should provide the resistance test, only then would patients be on the right medication.
It would save a lot of problems – also a lot of money.
Most of all – The misery that these medications cause. They are addictive and very difficult to withdraw from.
It needs a special clinic, experienced person to make sure the withdrawal is successful.
My son has two disabilities from the medication.
He is in a wheelchair for over 20 years suffering from TD – Tardive Dyskinesia from the medication – injury to the brain – spine (Clozapine) no dopamin in this system
Disability (Risperidone) – brain disturbance so now lacks capacity.
They only knew one thing – pills/Tablets.
The system needs to change. Put the right people in the right jobs.
Mental health destroys everything ? (The system).”
It is Elizabeth’s Birthday on Monday. She is 37, her life and mine ruined by NHS/social services. Police on the other hand have not acted unprofessionally towards us. All we have encountered under the NHS has dishonesty, bullying and cruelty. There is no sign whatsoever of the Oliver McGowan training. has been no decent communication towards us as a family. To deprive leave is cruelty. To take away every bit of enjoyment by locking away her mobile phone is cruelty. To pick on and bully a mother like me is nasty. I have been banned for months on end from visiting and am told I cannot visit the ward alone. In any case I do not feel safe to step foot alone in that place any more as they have called the Police out so many times are reporting adversely- writing notes during visits and God knows what is being said behind our backs. This is all aimed at me because I have dared to challenge but everyone goes along with what they are being instructed. It is not out of concern for the patient it is brutal bullying – that is what we or rather I have encountered. I have requested records under Data Protection only for my requests to be ignored and I have had to go to the ICO. There are no doubt awful things written behind my back and to call Police on so many occasions which makes you wonder what is being reported against you. Do they not even stop to think Police are busy and they are wasting Police time rather than try to make out they have cause to ask them to visit the ward. This is being done to threaten and bully me and deter me from making contact whilst they continue to hold my daughter a prisoner indefinitely. It is not done out of concern or kindness for the vulnerable patient who is suffering. The reason is I do not trust anyone working for LINOLNSHIRE PARTNERSHIP TRUST is that they are using the point that it is no individual person’s responsibility and that all the professionals agree with their actions which most certainly go against their code of conducts. My whole point is that the agencies assigned to protect seem to be doing nothing.
CQC have visited ward - then you get a letter and they do not want to get involved. The PHSO, LG Ombudsmen are other examples who dismiss a complaint they know full well they cannot defend. The defence is not towards you the public but towards the professionals.
The GMC, HCPC, GMC and NMC all protect the professionals.
Then there is the Professional Standards Agency who apparently have no powers to intervene. The Professionals Standards Agency are supposed to be responsible for overseeing all these agencies but I have just contacted them to hear they have no power under legislation to act. No wonder there is such unaccountability.
If there is no accountability what is the point of any codes of conduct or any of these agencies which cost the public a great deal of money yet fail to protect them/the vulnerable people. Iif nothing can be enforced to protect thousands of vulnerable people trapped in dreadful institutions and being abused all over this dreadful country then the Government surely needs to act. All the MP locally is contact the Trust. You will then get a standard letter and everything continues to go on and nothing is ever resolved so it is a waste of time. However our MP happens to be Health Secretary which is why I am turning to her not only for the sake of my daughter but so many others nationwide.
The most prominent people standing in the way of visits and contact appear to be DR WAQQAS KHOKHAR, the Responsible Clinician for Castle Ward and Emily Scott, Clinical Lead but then there are those at the very top namely Sarah Connery CEO, there is also the Management of the ward. Noone is taking the law into account and all hiding behind the MDT instead of being accountable individual or being made to review their actions according to their own code of conducts of which they are in breach. I am told not to contact the Carers Champion any more, all correspondence to be sent via the Care Concerns email address for which you do not get response when it comes to your questions as a whole.
From: Christopher Reid <Chris.Reid@parliament.uk> Sent: 22 January 2024 14:55 To: susanb255 Subject: Re: Letter from Sarah Connery via Victoria Atkins MP (Case Ref: VA18567)
Dear Ms Bevis,
Thank you for your response.
As you are aware, we have previously raised your concerns about the wider issues with mental health and families with Victoria’s ministerial team, We are still waiting to hear back from them about this, however will of course let you know as soon as we do.
of course if you change your mind and want us to go back to the Trust on your daughter’s specific case them please do let us know.
Yours Sincerely,
Christopher Reid Senior Caseworker Office of the Rt Hon Victoria Atkins MP Member of Parliament for Louth & Horncastle Secretary of State for Health and Social Care
House of Commons London SW1A 0AA
01507 527017
In line with data protection regulations, the Office of Victoria Atkins MP processes your personal data for casework and policy enquiry purposes. Please see our privacy notice at www.victoriaatkins.org.uk/privacy-notice.
________________________________________ From: susan bevis Sent: 22 January 2024 12:38 To: REID, Chris <chris.reid@parliament.uk> Subject: Re: Letter from Sarah Connery via Victoria Atkins MP (Case Ref: VA18567)
Dear Mr Reid
It is a waste of time going back to Trust Offices. I would like this whole issue of vulnerable people being sent far away from families out of area and kept a prisoner on MH wards for years and years dealt with in Parliament. This is Victoria’s area and I know other cases and there needs to be more options. Instead of bullying families and carers why not involve them in projects and set up something like Simon Trust. There needs to be something done about the MHA and MCA as this is being abused. There needs to be facility provision close to families and laws on accountability especially to Responsible clinicians who can lie as I can well and truly prove. There needs to be restriction on length of time spent on acute wards. When ms Connery speaks of 70 emails that is ridiculous. In East Lindsay there is hardly anything in terms of facilities.
I have not had anything in terms of satisfactory response. The court system too is a disgrace. Courts should be open and transparent.
I do not like to see human rights and other law being abused.
I would like to see more protection towards vulnerable people and their rights in hospitals and care homes and have been reading the paper just out on visiting rights etc.
All of this I would like to be addressed nationwide.
There needs to be accountability especial towards those at the top of Trusts and the Responsible Clinicians employed by a Trust. For instance it is wrong for staff by way of instructions to act ultra vires, to use severance of the tiniest bit of leave to hospital shop, to take phone away, to use police to threaten to discourage family contact and worst of all day things like “I am having to ban you indefinitely ms bevis on the grounds ************************* stated dr Waqqas Khokhar on 28 December 2023.
Regards
Susan Bevis
In all this time no Impact Assessment has been carried out. This is NHS Guidelines. Secondly the Government paper on visiting wards and care homes is completely forgotten by LPFT. They are rated good by the CQC and in all this time the CQC who describe themselves as a “business” have done nothing. The matter has also been referred to other agencies too responsibility for those employed by this Trust who say constantly “IT IS AN MDT DECISION” - No! it is not an MDT Decision if you read the details of their Code of Conduct. When I mention this they have no comment to say whatsoever and I am sure that many are just going along with instructions for the sake of their jobs.
I have nothing to hide which is why I am writing openly and honestly on here about the dreadful cruel and abusive NHS and how they treat the most vulnerable people in this country with no accountability whatsoever. When I say “how would you feel if you were treated this way and had every phone call listened to and people dutifully writing notes that are not nice no doubt behind your back.” It is both undignified and degrading. Also this punishment is affecting others in the family too.
Eizabeth has spent years held like a prisoner on acute wards by LINCOLNSHIRE PARTNERSHIP TRUST who launched a campaign of bullying. When you phone it takes ages to get through on the phone sometimes. You then speak to a nurse or HCA and they cannot put you through to the phone that we as a family pay for. This has been going on for a very long time now. I think the contact through Vodafone is something like £13 a month but there is no usage because Elizabeth’s phone is locked away and they try to make out that there is a policy in place that is the same for other people but that is not true. I know this because friends on the ward were helping Elizabeth to contact me.
Last night I phoned the ward. After three attempts of not even being able to hear Elizabeth finally I got to speak to her on the ward phone. Her phone is left uncharged in the locker and they try to make out that she has access to it. All the time LINCOLNSHIRE PARTNERSHIP TRUST is discouraging and blocking calls to her mobile in the most disgusting manner. All the time they get away with it because the CQC and other agencies involved who I will feature later on do absolutely nothing. In an area where we have encountered nothing but bullying it is easy to see why staff are afraid to speak up.
Subject: Epilepsy & Psychosis
If Elizabeth has epilepsy she should not be treated with prn benzos for rapid tranquilisation. Prolonged and repeated use of benzodiaepines can increase the risk of rebound seizures or interictal epileptiform discharges (IEDs) in some individuals.
Schizophrenia-like symptoms are observed in some patients and are associated with epileptiform discharges but not overt seizures. The good response to antiepileptic treatment could be interpreted in the context of a (para)epileptic pathomechanism.
“The EEG alterations might be due to a polygenetic effect due to different genes”.
This is why accurate diagnosis is so important. You will see in the case below that a patient with schizophrenia like symptoms had epilepsy and recovered when taken off antipsychotics and treated with anti-convulsants.
The idea that schizophrenia is ‘confirmed’ by daily observations conducted by unqualified staff is absurd. Care assistants cannot possibly know how to differentiate between IEDs and psychosis induced by other causes. This is why PANSS and associated physiological testing is crucial. LPFT are in the dark ages when it comes to diagnosing and treating psychiatric patients. They neglect proper investigation of genetic markers in psychosis, they neglect EEG examination, they neglect genetic testing for treatment refractivity, they neglect investigation the potential inflammatory causes of brain disturbances and the ignore ADRs.
This indicates an ideological approach to diagnosing and treating psychosis rather than a medical one. Belief based medicine, not evidence based medicine.
See paper below. It has some interesting comment on Clozapine you may like. Reference 16 in the bibliography is to a paper that indicates that Clozapine can actually induce epilepsy in some patients due to a genetic polymorphism. LPFT do not test for that either.
Schizophrenia Associated with Epileptiform Discharges without Seizures Successfully Treated with Levetiracetam
1Section for Experimental Neuropsychiatry, Department of Psychiatry, Faculty of Medicine, University of Freiburg, Freiburg, Germany
2Freiburg Epilepsy Center, Department of Neurosurgery, Faculty of Medicine, University of Freiburg, Freiburg, Germany
3Department of Rheumatology and Clinical Immunology, Faculty of Medicine, University of Freiburg, Freiburg, Germany
Background: Schizophrenia-like disorders can be divided into endogenic or primary, idiopathic, polygenetic forms, and different secondary, organic subgroups [e.g., (para)epileptic, immunological, degenerative]. Epileptic and paraepileptic explanatory approaches have a long tradition due to the high rate of electroencephalography (EEG) alterations in patients with schizophrenia.
Case presentation: We present the case of a 23-year-old female patient suffering, since the age of 14 years, from a fluctuating paranoid-hallucinatory syndrome with formal thought disorder, fear, delusions of persecution, auditory, visual, and tactile hallucinations, as well as negative and cognitive symptoms. Laboratory measurements showed increased titers of antinuclear antibodies (ANAs) in the context of ulcerative colitis. While there was no clear history or evidence of epileptic seizures, the EEG showed generalized 3 Hz polyspike wave complexes. Under treatment with levetiracetam, the symptoms disappeared and the patient was able to complete vocational training.
Conclusion:The schizophrenia-like symptoms associated with epileptiform discharges but not overt seizures and the good response to antiepileptic treatment could be interpreted in the context of a (para)epileptic pathomechanism. The EEG alterations might be due to a polygenetic effect due to different genes. Mild immunological mechanisms in the framework of ulcerative colitis and increased ANA titers might have supported the network instability. This case report illustrates (1) the importance of EEG screenings in schizophrenia, (2) a potential pathogenetic role of epileptiform discharges in a subgroup of patients with schizophrenia-like symptoms, and (3) that antiepileptic medication with levetiracetam could be a successful treatment alternative in schizophrenia-like disorders with EEG alterations.
Background
Schizophrenia-like disorders are characterized by delusional perception and delusions of control, hallucinations (e.g., commenting or discussing voices), thought insertion or withdrawal, cognitive impairment, thought disorders, or social withdrawal.1 In addition to primary, endogenic or idiopathic, polygenetic forms, different secondary pathophysiological mechanisms [e.g., (para)epileptic, immunological, degenerative] can be assumed. Because of the high rates of electroencephalography (EEG) alterations, ranging from 7 to 60% in patients with schizophreniform syndromes, epileptic and paraepileptic explanatory approaches have a long tradition (1–3). In line with this assumption, we reported the first case of a young patient with a schizophrenia-like disorder, generalized spike-and-slow-wave complexes without epileptic seizures but with remission under treatment with valproate (4, 5). Immunological reasons might be due to autoantibody-associated autoimmune encephalitis, cerebral vasculitis, or collagenosis [e.g., systemic lupus erythematosus (SLE)] (6). Immunological effects might lead to network instability and therefore cause (para)epileptic phenomena (7).The detection of a (para)epileptic or immunological mechanism opens new treatment perspectives, in that antiepileptics or immunomodulators may be helpful (4, 5, 7–10).
Case Presentation
Clinical Presentation
We present the case of a 23-year-old female office clerk suffering from fluctuating paranoid-hallucinatory symptoms since the age of 14 years (2007). Therefore, the diagnosis of paranoid schizophrenia was made by different psychiatrists. Although taking neuroleptics, in the course of the disease, the patient developed five episodes (for several weeks) with paranoid-hallucinatory exacerbation. In these episodes, the patient suffered from formal thought disorder, fear, delusions of persecution, auditory hallucinations with commenting, discussing, and commanding voices, visual hallucinations with seeing maggots in her room, and tactile hallucinations with the feeling of being touched from behind. In parallel to these exacerbations, the patient developed severe negative and cognitive symptoms including attention and memory deficits, fatigue, depressive mood, and sleep disturbances thus completing the psychopathological features of comprehensive schizophrenia. Neurological and medical examinations were normal.
Family History
There was a positive family history for unipolar depression, which was diagnosed earlier in two sisters, both parents, and both grandmothers. There was no history for schizophrenia-like psychopathology, bipolar disorder, or epilepsy.
Somatic and Developmental History
Symptoms started 6 weeks after pain of the large joints. Therefore, a rheumatological disease was discussed. During an external work-up of repeated diarrhea, a chronic inflammation gut disease (ulcerative colitis) was diagnosed in 2014 and treated with mesalazine. No birth complications or in utero abnormalities were remembered; the birth was performed by cesarean section. The early childhood development was normal. No febrile convulsions or inflammatory brain diseases were remembered. The patient suffered mild cerebral contusions at the age of 4 and 12 years.
Diagnostic Findings
The diagnostic findings are summarized in Table 1. Taken together, the immunological alterations were compatible with the previously known ulcerative colitis (11). The electrophysiological findings (Figure 1) would be compatible with primary (idiopathic) generalized epilepsy; however, the history for epileptic seizures including absences and myoclonic jerks was negative.
Table 1
Figure 1. Frontal accentuated intermittent rhythmic delta activity (FIRDA, left) and generalized 3 Hz polyspike wave complexes (middle) in the bipolar longitudinal rows (7 µV/mm, 0.3 s, 70 Hz). The findings of the independent component analysis are presented in the right picture [the following four relevant components were found, left: activity traces, with examples of atypical activity cut from the clinical electroencephalography and appended at the dotted lines. Right: topographies, nose upward, negative (direction opposite of activity trace) blue, positive (direction same as activity trace) red. Right (component 3) and left (component 5) frontal activity show most prominent ~2.6 Hz bursts. Higher frequency activity frontocentral (component 2) and occipital (alpha component 7) are partially related].
Differential Diagnosis
The schizophreniform symptoms fulfilled the criteria of paranoid-hallucinatory schizophrenia (see footnote 1). Therefore, the most important differential diagnoses would be schizophrenia plus coincidental epileptiform discharges. Although the findings of the investigation led us to our consideration of neuropsychiatric SLE, the American College of Rheumatology classification criteria for SLE were not fulfilled.2
Therapy and Outcome
External neuroleptic treatment with risperidone (4 mg), amisulpride (600 mg), perazine (100 mg), aripiprazole (15 mg), and clozapine (275 mg) did not lead to long-term stabilization. Additional treatment with fluoxetine (20 mg) and citalopram (20 mg) for affective, negative, and cognitive symptoms did not successfully improve these symptoms. During the first visit in our clinic, in 2013, we detected the abovementioned epileptiform discharges. Assuming a (para)epileptic pathomechanism, we added antiepileptic treatment with valproate (1,500 mg) to the neuroleptic medication with clozapine and aripiprazole. At this point, the cognitive deficits improved significantly. Also, the EEG improved except for the (F)IRDAs. Another paranoid-hallucinatory episode in 2014 was treated successfully with a dose increase of clozapine and valproate. Because of a strong weight gain, the therapy with valproate was changed to topiramate (200 mg) in 2014. Assuming a (para)epileptic pathomechanism, clozapine was reduced and stopped in 2014. Aripiprazole was reduced in January 2014 and stopped in 2015. Normal results were found in both the routine EEG and in the EEG after sleep deprivation (2014). In the further course, topiramate led to a severe loss of appetite and was therefore changed to levetiracetam (1,500 mg) in 2014. The mental condition stabilized with the short-term antiepileptic treatment with topiramate and the subsequent antiepileptic treatment with levetiracetam (since 2014, and since 2015 as monotherapy). There were no more paranoid-hallucinatory episodes, the negative symptoms declined, the patient became a mother (in the spring of 2016); she lived alone, took care of her daughter, and simultaneously finished her vocational training (in the summer of 2016). She was able to suspend the mesalazine therapy and therefore only took levetiracetam (1,500 mg) at the time of stabilization.
Discussion
We present the case of a patient with a schizophrenia-like disorder and, following our judgment, a (para)epileptic pathomechanism, because of the distinct epileptiform discharges without seizures and remission under the anticonvulsive treatment with topiramate and subsequently levetiracetam monotherapy.
Reason and Potential Pathophysiology of Network Instability
The EEG alterations might be due to a polygenetic effect caused by different genes (12). The immunological mechanisms in the framework of ulcerative colitis and increased antinuclear antibody titers might have supported the network instability by mild inflammatory processes (7, 13–15). Medication might also disclose underlying polygenetic or immunological network instability (16). The local area network inhibition (LANI) hypothesis might explain the causal relationship between epileptiform EEG discharges and schizophrenia-like symptoms. Excitatory network activity, as represented by the 3 Hz polyspike wave complexes, might lead to consecutive inhibitory processes in a physiological attempt of the central nervous system to stabilize the excitatory–inhibitory equilibrium of local cerebral networks. The repetitive excitatory activity, as documented by consecutive EEGs in our patient, could have exceeded a critical threshold, leading to the successive hyperinhibition of cerebral networks. Following the LANI hypothesis, the symptoms are due to the secondary induced processes of hyperinhibition (e.g., temporal hyperinhibition might have led to auditory hallucinations or memory deficits) (2–5, 17).
Treatment Considerations
Following the LANI hypothesis, the cognitive improvement after the addition of valproate to the neuroleptic treatment would be explained by the reduced epileptic activity and therefore the subsequent amelioration of inhibitory processes. In line with this assumption, comprehensive long-term stabilization was not achieved by several attempts of neuroleptic medication alone in spite of clear and very convincing effects of the treatment with clozapine in particular on positive symptoms. However, such a comprehensive improvement and even full remission was achieved with topiramate and later levetiracetam monotherapy. Thus, clozapine with its well-known proconvulsive properties might well have counteracted inhibitory processes, while it is at the same time most likely unable to improve causative excitatory neuronal activity. By contrast, by reducing the epileptiform activity, topiramate and levitiracetam monotherapy might have resulted in a more causal and therefore more comprehensive improvement of relevant pathophysiology. Earlier, we published a case of a (para)epileptic schizophrenia-like disorder successfully treated with valproate (4). Valproate, and likewise lamotrigine, is already established as an augmentative treatment strategy in schizophrenia (18). One might hypothesize that patients with (para)epileptic pathomechanisms will benefit significantly more from antiepileptic treatment than other subgroups. To our knowledge, this is the first published case study that describes a patient with a schizophrenia-like disorder who was successfully treated with levetiracetam. Levetiracetam is rarely used off-label in psychiatry probably because of its potential side effects, such as agitation, aggression, fear, and psychosis (2). The advantage of levetiracetam is that it can be rapidly dosed up to effective concentrations. Therefore, on a single case basis, the working hypothesis of a (para)epileptic pathomechanism could be tested quickly. In comparison, valproate effects could be due to combined γ-aminobutyric acid (GABAergic) and antiglutamatergic effects, and lamotrigine effects might be due to potential antiglutamatergic effects. However, the mechanism of levetiracetam cannot be explained by such direct transmitter effects. The effects of levetiracetam seem to be associated with the binding of the synaptic vesicle glycoprotein 2A (SV2A) (2). SV2A can be found in presynaptic membranes; it controls the calcium-dependent exocytosis of different neurotransmitters into the synaptic gap (19, 20). Therefore, it might also influence GABAergic and glutamatergic transmission (21).
Limitations
Epileptiform discharges are found in less than 1% of healthy adults (1, 22–24) and as a rare consequence of clozapine treatment (16). Therefore, the EEG alterations could be interpreted either as an incidental finding in a patient with schizophrenia or as a clozapine side effect. However, the clinical course—with improvement under antiepileptic treatment in parallel with EEG normalization—speaks against the assumption. The pathophysiological processes might be explained by the LANI hypothesis; however, this is only an unproven, theoretical framework that needs further investigation.
Conclusion
This case report illustrates the idea of a possible (para)epileptic pathomechanism in a patient with a schizophrenia-like disorder. Regarding diagnostic procedure, our case shows the importance of EEG examinations in typical schizophrenia-like disorders. Regarding pathophysiology, the case illustrates a potential pathogenetic role of epileptiform discharges in a subgroup of patients with schizophrenia-like symptoms. Regarding treatment, the case demonstrates that anticonvulsive medication with levetiracetam and also topiramate or valproate could be a successful treatment alternative in schizophrenia with EEG alterations.
Ethics Statement
The patient has given her informed and written consent for this case report, including the presented images, to be published.
Author Contributions
LTvE treated the patient. DE wrote the paper and performed the data collection. DE and LTvE performed the interpretation of the diagnostic findings and therapy effects. BF performed and interpreted the EEG analysis. NV performed and interpreted the immunological analyses. EP and D-MA reviewed the diagnostic results and contributed to the manuscript preparation. All the authors were significantly involved in the theoretical discussion and the preparation of the manuscript, and they read and approved the final version of the manuscript.
Conflict of Interest Statement
DE, EP, and BF: none; D-MA: lecture fees from UCB Pharma; NV: advisory boards, lectures, research, or travel grants within the last 3 years: Janssen-Cilag, Roche, Novartis, AbbVie, GSK, and Medac. LTvE: lectures, work shops, or travel grants within the last 3 years: Eli Lilly, Medice, Shire, UCB, Servier, and Cyberonics.
Abbreviations
ACR, American College of Rheumatology; ANA, antinuclear antibody; CSF, cerebrospinal fluid; EEG, electroencephalography; FIRDA, frontal intermittent rhythmic delta activity; GABA, γ-aminobutyric acid; HV, hyperventilation; ICA, independent component analyses; IRDA; intermittent rhythmic delta activity; LANI, local area network inhibition; SLE, systemic lupus erythematosus; SV2A, synaptic vesicle glycoprotein 2A.
1. Shelley BP, Trimble MR, Boutros NN. Electroencephalographic cerebral dysrhythmic abnormalities in the trinity of nonepileptic general population, neuropsychiatric, and neurobehavioral disorders. J Neuropsychiatry Clin Neurosci(2008) 20:7–22. doi: 10.1176/appi.neuropsych.20.1.7
2. Tebartz van Elst L, Perlov E. Epilepsie und Psyche: Psychische Störungen bei Epilepsie – epileptische Phänomene in der Psychiatrie. 1st ed. Stuttgart: Kohlhammer (2013).
3. Endres D, Perlov E, Feige B, Fleck M, Bartels S, Altenmüller D, et al. Electroencephalographic findings in schizophreniform and affective disorders. Int J Psychiatry Clin Pract (2016) 16:1–8. doi:10.1080/13651501.2016.1181184
4. van Elst LT, Schulze-Bonhage A, Altenmüller D, Ebert D. Generalised spike-and-slow-wave complexes without seizures in schizophrenia. Br J Psychiatry (2011) 199:253–4. doi:10.1192/bjp.199.3.253a
5. Tebartz van Elst L, Krishnamoorthy ES, Schulze-Bonhage A, Altenmüller D, Richter H, Ebert D, et al. Local area network inhibition: a model of a potentially important paraepileptic pathomechanism in neuropsychiatric disorders. Epilepsy Behav (2011) 22:231–9. doi:10.1016/j.yebeh.2011.06.016
7. Tebartz van Elst L, Stich O, Endres D. Depressionen und Psychosen bei immunologischen Enzephalopathien. PSYCH up2date (2015) 9(05):265–80. doi:10.1055/s-0041-102941
9. Endres D, Perlov E, Stich O, Rauer S, Waldkircher Z, Lange T, et al. In vivo hypoglutamatergic state is associated with reduced cerebral glucose metabolism in anti-NMDA receptor encephalitis. BMC Psychiatry (2015) 15:186. doi:10.1186/s12888-015-0552-4
10. Endres D, Perlov E, Stich O, Tebartz van Elst L. Steroid responsive encephalopathy associated with autoimmune thyroiditis (SREAT) presenting as major depression. BMC Psychiatry (2016) 6:184. doi:10.1186/s12888-016-0897-3
13. Hazouard E, Legras A, Diot E, Ferrandière M, Corcia P, Giniès G. [Cerebrospinal fluid complement and antinuclear antibodies in lupus meningoencephalitis]. Rev Neurol (Paris) (1998) 154:549–50.
14. Bonrath E, Rijcken E, Dziewas R, Vieth V, Bettenworth D, Senninger N, et al. [Cerebral vasculitis as rare extraintestinal manifestation in ulcerative colitis: review of the literature and case report]. Zentralbl Chir (2010) 135:350–3. doi:10.1055/s-0030-1247464
17. Tebartz van Elst L, Fleck M, Bartels S, Altenmüller D, Riedel A, Bubl E, et al. Increased prevalence of intermittent rhythmic delta or theta activity (IRDA/IRTA) in the electroencephalogram (EEG) of patients with borderline personality disorder. Front Behav Neurosci (2016) 10:12. doi:10.3389/fnbeh.2016.00012
18. Dold M, Leucht S. Pharmacotherapy of treatment-resistant schizophrenia: a clinical perspective. Evid Based Ment Health (2014) 17:33–7. doi:10.1136/eb-2014-101813
19. Lynch B, Lambeng N, Nocka K, Kensel-Hammes P, Bajjalieh S, Matagne A, et al. The synaptic vesicle protein SV2A is the binding site for the antiepileptic drug levetiracetam. Proc Natl Acad Sci U S A (2004) 101:9861–6. doi:10.1073/pnas.0308208101
20. Zhang L, Li S, Li H, Zou X. Levetiracetam vs. brivaracetam for adults with refractory focal seizures: a meta-analysis and indirect comparison. Seizure (2016) 39:28–33. doi:10.1016/j.seizure.2016.05.004
21. Wood MD, Gillard M. Evidence for a differential interaction of brivaracetam and levetiracetam with the synaptic vesicle 2A protein. Epilepsia (2016). doi:10.1111/epi.13638 [Epub ahead of print].
24. Thorner MW. Procurement of electroencephalograph tracings in 1000 flying cadets for evaluating the Gibbs technique in relation to flying ability. USAD School of Aviation Medical Research Report No. 7–1. (1942).
Citation: Endres D, Perlov E, Feige B, Altenmüller D-M, Venhoff N and Tebartz van Elst L (2017) Schizophrenia Associated with Epileptiform Discharges without Seizures Successfully Treated with Levetiracetam. Front. Psychiatry 8:12. doi: 10.3389/fpsyt.2017.00012
Received: 27 October 2016; Accepted: 17 January 2017; Published: 08 February 2017
The PANSS has been studied for its psychometric properties, and the data shows adequate Internal consistency, good test-retest reliability, and inter-rater reliability. In addition the PANSS has been researched in quality of life studies, functional status, natural history of schizophrenia and treatment outcomes. It has most of its evidence base to support its use for grading the severity of schizophrenia symptoms, staging of schizophrenia and treatment progress with medications.
The scale has mostly been used to inventory, grade and follow the symptoms in schizophrenia. It quantifies positive symptoms, which refer to an excess or distortion of normal functions (e.g., hallucinations and delusions), and negative symptoms, which represent a diminution or loss of normal functions. The PANSS is composed of 3 subscales: Positive Scale, Negative Scale, and General Psychopathology Scale. Each subscale is rated with 1 to 7 points ranging from absent to extreme. The range for the Positive and Negative Scales is 7-49, and the range for the General Psychopathology Scale is 16-112. The total PANSS score is simply the sum of the sub scales. In addition to these measures, a Composite Scale is scored by subtracting the negative score from the positive score. This yields a bipolar index that ranges from –42 to +42, which is essentially a difference score reflecting the degree of predominance of one syndrome in relation to the other.
The Positive and Negative Syndrome Scale (PANSS) was published in 1987 by Stanley Kay, Lewis Opler, and Abraham Fiszbein. It’s a scale used for measuring symptom severity of schizophrenia, and widely used in the study of psychopharmacologic therapy. The scale was based off the Psychopathology Rating Schedule (PRS) and the Brief Psychiatric Rating Scale (BPRS). The PANSS is a 30-item clinician-administered rating scale, but requires 45 to 50 minutes to be administered by a subject matter expert. The interviewer must be trained to a standardized level of reliability. The PANSS has been published officially across 40 languages and is used internationally in mostly clinical research.
PANNS is also used to deny patients autonomy (capacity) It is used to judge the diminution of loss of function by rating it on a scale. If LPFT do not use this scale how have they determined that ****** lacks capacity? LPFT state she has severe symptoms but have not measured them. The severity or otherwise seems to be based on the opinions of staff, some of whom are not medically qualified, never mind ‘subject matter experts’.
This is why the PANSS score is important. I do not need to agree with the diagnostics of schizophrenia to see the importance. The fact is that ****** been diagnosed with paranoid schizophrenia but LPFT have not used this metric in the diagnosis or the treatment they give her. LPFT prefer and have stayed reliant on subjective observations by multiple staff on a daily basis which is hardly a scientific method and effectively is a trial and error, hit and miss approach. PANSS is a doctors responsibility, not a ward care assistant’s.
Note that medication decisions are based on PANSS and so I am curious to know what are LPFT using in that case?
This is very similar to the ignoring of the metabolism issues. Whilst known that she is a poor metaboliser, :LPFT make no provision for it. So, they take no notice of the diagnostic criteria or notice of metabolism problems yet still label ****** with this ‘diagnosis’ and medicate her according to it being correct?
It has come to my attention the following:
“****** regular mental health medication is a Clopixol (Zuclopenthixol Decanoate) 400mg depot. This is administered once every two weeks and has been authorised by a Second Opinion Appointed Doctor on 29th December 2023 as well as being supported by ******** Responsible Clinician.
-LPFT does not routinely use the Positive and Negative Syndrome Scale for Schizophrenia (PANSS). This was confirmed by the Responsible Clinician who has stated that ******** progress is currently being judged based on engagement with staff and activities.”
Finally I do not appear to have response to my previous email about visiting the ward on the 12 February and ****** phoned me today. Please explain about Sheffield. I was not clear whether this is another placement or what? ****** has shared with me she is thought to have epilepsy and that Dr S came to see her. Can you please advise how things went and the outcome? ****** said that it was needed a recording of the episode which she had another one the other day. It is not good that my daughter is injected after every episode. This is affecting her sleep pattern and it is affecting her blood oxygen levels. Rapid tranquilisations on a frequent basis are not good for my daughter’s physical health and may even be causing the problem of episodes rather than suggestions that I am contributory. I have not been allowed to see ****** for months so how can this be any way contributory to me? On the Advanced Declaration it clearly says that ****** does not wish to be subject to unnecessary treatments and rapid tranquilisations fit into that description. Please note that the rapid tranquilisations are not part of my daughter’s “treatment” and should therefore cease. I do not want to hear that everything has been agreed by the SOAD. In fact the SOAD needs to be aware of the above and so do the CQC.
I would suggest that LPFT contact Cygnet Durham where Dr M was witness to such episode as there may be a recording of that under Cygnet.
As someone who has attained qualifications re Best Interest I can now judge that nothing has been done correctly under LPFT, especially the capacity assessments along with the PANSS score.
From: susan bevis Sent: 07 February 2024 22:45
To: CARECONCERNS (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST) <lpft.careconcerns@nhs.net>
Cc: Enquiries <Enquiries@cqc.org.uk>
Subject: PANSS SCORE – *********** – For the Attention of Sarah Connery, Kevin Lockyer and Emily Scott (Clinical Lead)