Mental Health Act Administration Office
Trust Headquarters
St Georges
Long Leys Road
LINCOLN LN1 1FS
20 October 2023
In Confidence
Mrs Susan Bevis
Dear Mrs Bevis
We have been informed about an incident that took place in Reception at Trust Headquarters, St Georges Site on Wednesday 18th October 20233, in which you presented as hostile and aggressive, demanding immediate access to a senior manager
As an employer LPFT has a duty of care for the health, safety and wellbeing of its staff. We also have a legal responsibility to provide a safe and secure working environment for staff. Staff mental health is as important as their physical health. Any incident in which an employee is abused, threatened or assaulted in circumstances relating to their work is unacceptable and not tolerated. This includes the serious or persistent use of verbal abuse, aggressive tone or language and swearing.
In accordance with NHS guidance, such behaviour is not acceptable and you are now formally warned that if there is a repeat of this or similar behaviour again in the future at any LPFT site the Police will be called to escort you from Trust premises.
Going forward please ensure that you only attend Castle Ward for your pre-booked appointment times once a week. This will allow ward staff to facilitate the visits as directed by Elizabeth’s Responsible Clinician as part of the plan for her care and treatment; please be assured that these decisions have not been made by staff in Trust Headquarters or other teams and will be reviewed regularly. Unannounced visits to Castle Ward to see Elizabeth will not be able to be facilitated.
Yours sincerely
THE MENTAL HEALTH ACT AND LEGAL TEAM
CHAIR KEVIN LOCKYER
CHIEF EXECUTIVE: SARAH CONNERY
VISIT TO ELIZABETH ON 30 OCTOBER 2023
There is no greater bullying and abuse of power than to deprive contact with your vulnerable relative. LPFT have most certainly achieved this. Threats and defamation of character are another way to bully one person and then to carry out safeguarding behind your back. This was already done under Enfield and both Trust and Council were forced to apologise. Here under LPFT this is going on against me because it only takes one complaint and then everyone gangs up yet when I asked for safeguarding this was dismissed and ignored especially when so many other patients had come up to me in the grounds to tell me about my daughter’s shocking treatment and frequent rapid tranquilisations that led to a bad accident that we the family have only just got to hear about via Elizabeth.
I had to sit outside on the floor for the entire visit whilst only a friend was allowed to visit unescorted who actually booked the visit and made it clear it was for both of us but I did not argue as they would have called security or Police once again. I could only see Elizabeth for about 5 minutes because apparently it was ordered that I needed to have 2-1 supervision. Nurse Paul Tarling told me to leave the ward and I did so immediately when ordered. The reason was there was nothing written down in their books about me coming and they were short staffed and could not provide 2-1 supervision. The staff on Castle Ward point to Trust HQ but it is very clear who is behind this decision. The unsigned letter from Trust HQ explains in the last paragraph. I am still waiting for the CCTV footage requested under GDPR Rules and nothing previously has ever been produced despite similar comments alleging threatening abusive behaviour on my part. I have written to the records department of LPFT and requested CCTV footage along with an accompanying friend.
Email dated 31.10.23 regarding visit 30.10.23 by accompanying friend the following was written:
“I arranged this meeting myself to accompany Susan Bevis to Castle Ward on the above date. I clearly pointed out that the visit would be both of us verbally.
We arrived yesterday at 6.00 pm and were allowed onto the ward and Elizabeth was with us in the visiting room unescorted. However, a male nurse, I understand his name is Paul Tarling appeared in the visitors room and announced that only 1 visitor had been agreed and this was myself to which I responded that I had requested Susan Bevis to visit alongside me and was advised this was noted in the visitor’s book.
Anyway Susan Bevis was told to leave the ward and sat outside where she remained seated on the floor just outside the ward whilst my visit continued unescorted.
I am concerned at the effect this may all be having on Elizabeth and her care. It is clear there is personal vendetta from Dr Waqqas Khokhar towards Susan Bevis and I understand he has described her as being “a bad influence”. I am also aware that previously there were incidents not substantiated by CCTV or recordings and that it is awaited proof of alleged threatening behaviour on the part of Susan Bevis during her visit to Trust HQ with CM (another friend).
Whilst the nurse (Paul Tarling) said it was not a ward decision I can see quite clearly from the letter Susan Bevis shared with me attached that it is clearly a decision made by you, Dr Khokhar. I therefore would like to understand further why such restrictions are in place and to understand Trust Policy on banning visitors and restricting contact.
Perhaps you or Ms Munro can send me the Trust Guidelines and Policy in this respect.
I would also like to know the time of the meeting on the 3rd November I have heard all about. Perhaps you can send me the link to this meeting so we can all take part.”
Yours sincerely
My email to Ms Ann Munro
From: susan bevis
Sent: 31 October 2023 21:18
To: CARECONCERNS (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST)
Cc: Enquiries; Parliamentary Health Ombudsman
Subject: FAO ANN MUNRO ENQ 17716124293
Dear Ms Munro
Thank you for your letter of 30 October.
CP11 Policy has been requested under FOI on 8 October 2023. I am also aware Elizabeth has been shown on screen the information she told me she had requested in written form.
I receive an invitation to attend Teams Meetings automatically but on two occasions have not been admitted. I have even phoned to advise of this. This is why I came in person on the 18th October and this had been prior arranged. Elizabeth was well aware and happy for me to attend and was looking forward to a repeat of the two hour leave granted. This was no ward round as it was held in the visitor’s room instead. I am also aware that Elizabeth absolutely hates these meetings where so many strangers attend, without any family members invited. She often chooses not to attend and quite often no advocate present.
I have another invitation for Teams ward round for the 1st November but am aware that there is a family meeting on the 3rd November and have not received the invitation to that? Am I going to be cut out of both meetings as has been the case for the most part?
To: KHOKHAR, Waqqas (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); TANIMOWO, Adekiite (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); KHOKHAR, Waqqas (LEICESTERSHIRE PARTNERSHIP NHS TRUST); CALDERONCARHUARICRA, Katteryne (BARNET, ENFIELD AND HARINGEY MENTAL HEALTH NHS TRUST); BARFORD-COWLEY, Amelia (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST) Cc: AITKENHEAD, Angela (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); Barker, Robert (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); Barlow, Diane (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); BELLAMY, Charlotte (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); CAMSELL, Lucy (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); FISHER, Bridgette (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); Fitzpatrick, Brenda (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); FLETCHER, Sue (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); GOSTELOW, Joby (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); JAQUES, Anthony (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); Keogh, Sophie (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); LAKE, James (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); MARABADA, Ngonidzashe (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); MOONS, Kashmir (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); POPOOLA, Tomilayo (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); SCOTT, Emily (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); SENDALL, Jackie (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); Skelton, Alice (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); SUNDAR, Siddharth (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); Tarling, Paul (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); Waby, Lucieann (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); WALLACE, Sarah (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); White, Jocelyne (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); Woodlock, Emma (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST); KAJUE, Hannah (BARNET, ENFIELD AND HARINGEY MENTAL HEALTH NHS TRUST); Lisa Anderson; susanb255@outlook.com; THORNTON, Andrea (NHS LINCOLNSHIRE ICB – 71E); PANDURANGI, Disha (LINCOLNSHIRE PARTNERSHIP NHS FOUNDATION TRUST)
Microsoft Teams Meeting
01 November 2023 10:40 – 11:00 (was 25 October 2023)
As you can see I am automatically included in Teams Meetings so it is not an excuse to say the Team would not have been aware of my invitation. See above – my email address is clearly on the list and would be seen as who is waiting to be let in for the meeting.
I am aware that there is another meeting on the 3rd November and have not received the link for that and neither has ****
No, your explanations have not reassured me in the slightest bit.
Whilst writing I have been reading with interest LPFT’s Policy
Just to reflect LPFT had three capacity assessments done each and every one of them flawed. They launched a campaign on bullying against me trying to take away POA for Health and Welfare then displacing me as NR and have had these 3 capacity assessments done in-house – two by doctors, one completely redacted and the other by an AMHP. They wanted them to show “no capacity” so that they could take over the life of my daughter who was not even sectioned before under the former area of Enfield. They have abused her rights and treated her like a restricted prisoner for over two years. There have been 10 doctors and 5 institutions and now they are looking for a 6th option and former area of Enfield cannot find any nearby option apparently. There has been no regard to Elizabeth’s feelings whatsoever and no regard to her family. There is a culture of bullying under LPFT as there was with Enfield and zero accountability. No consideration to human rights whatsoever and the wishes of my vulnerable daughter and she is not alone as there are countless others trapped in institutions such as this and treated as prisoners. She was not even on a section before we moved to Lincolnshire for the purpose of providing a nice home in the form of a small bungalow in our back garden. I moved to bring her closer to other family members. LPFT are not only in breach of human rights law but their only Policy and code of conduct and under the MHA too and should apply the least restrictive care but it has been the complete opposite.
“If an individual lacks the capacity to consent to admission and the admission is completed using the best interest framework then this should be recorded as per policy 6b and an urgent authorisation for a Deprivation of Liberty should be submitted to the Supervisory Body as per the MCA Policy 6b.
Is/was 6b applicable from Ash Villa to date? This being in addition to MHA (s3) detention. Surely LPFT would not have applied DoLs on account of the three flawed capacity assessments? If Dols in place is this the reason that Elizabeth has been treated like a restricted prisoner all along and denied leave and family contact for the most part? I did not think you could apply DoLs whilst held under S3 MHA or has anything changed?
LPFT POLICY
8.7 Visitors to LPFT Premises LPFT considers the safety and dignity of all visitors to its premises as extremely important. The link below provides guidance and procedures regarding the management of all visitors to Trust premises and includes process for managing visits by children: Please refer to visitors process within safeguarding policy 11
Was the reason for my “treatment” yesterday because safeguarding has been applied against me? Or was it simply a matter of being short staffed in order to accommodate 2-1 supervision as would apply in prison. If there are no staff to supervise 2-1 then this could leave problems with future visits and result in a similar scenario when I was told to leave the ward in front of Elizabeth, having just arrived, when the visit was booked including myself yet disputed and on account of staff shortages not permitted so it would seem. Please explain the reasons why 2-1 supervision applied against me and surely Elizabeth would be entitled to see family members in privacy as stated within your own Policy.
In November 2006 the Department of Health launched a ‘Dignity in Care’ campaign with an aim to put dignity and respect at the heart of care services, which extended into Mental health Services in 2007; and is now applicable in all health and social care settings. This campaign, led by the National Dignity Council, identified a 10 point Dignity Challenge to organisations which remains fully applicable today as follows:
6. Respect people’s right to privacy
8. Engage with family members and carers as care partners
9.4.1 Privacy refers to freedom from intrusion and relates to all information and practice that is personal or sensitive in nature to an individual.
9.4.2 Dignity refers to how people feel, think and behave in relation to the worth or value of themselves and others. To treat someone with dignity is to treat them as being of worth, in a way that is respectful of them as a valued individual. In care situations, dignity may be promoted or diminished by the physical environment, the organisational culture, by the attitudes and behaviour of the care team and others; and by the way in which activities are carried out.
Dignity applies equally to those service users (patients) who have capacity and to those who lack capacity.
9.4.3 Maintaining a service user’s (patient’s) privacy, dignity and respect is central to the delivery of effective health and social care, working in partnership with service users (patients) and where appropriate their carers / families.
OR
Do the above points not apply when the Trust sees someone as having no capacity and invoke their own measures of Best Interest regardless of any consideration towards Lynsey or her visitors/family?
9.4.4 Since July 2016 all organisations that provide NHS care or adult social care are legally required to follow the Accessible Information Standard. Meeting the standard requires workers across the Trust to ensure people who have a disability, impairment or sensory loss are provided with information that they can easily read or understand with support, so they can communicate effectively with health and social care services.
9.4.5 The following are examples of how to maintain a service user’s (patient’s) privacy and dignity:
9.9.2 Divisional Managers, Quality Assurance Leads and Team Leaders for in-patient services Divisional Managers, Quality Assurance Leads and Team Leaders for in-patient services are responsible for:
• Monitoring compliance with this policy
• Ensuring timely reporting of any non-compliance of this policy through the DATIX incident reporting system.
• Investigating any reported non-compliance with this policy
• Implementing any actions required following audits, incidents or patient / carer / worker feedback relating to Privacy, dignity and mixed sex accommodation. This may include individual worker development where there is evidence of failure in respect of related practice.
• Ensuring workers are aware of this policy, its content, where to access it; and their individual related responsibilities.
• Ensuring timely reporting of any non-compliance of this policy through the DATIX incident reporting system.
• Ensuring service user/s (patient/s) and their carers (where appropriate) receive an apology and an explanation of the reason for the breach.
• Investigating any reported non-compliance with this policy, including taking corrective action to prevent any recurrence.
• Actively promoting the service user’s (patient’s) privacy and dignity at all times.
Staff must acknowledge that the carer is frequently the person who knows the service user best, often having regular contact over many years throughout many changes in mental health well-being, social networks and professional support.
The carer is often the person who has to offer support during out-of-hours crises, which can be stressful. By involving the carer in the development of the care plan and crisis plan where appropriate, or ensuring they have a copy of it, the carer can feel supported in assisting the service user to follow it.
• An exchange of appropriate information with all relevant people, including carers
• Service users, families and carers are actively involved in, and remain informed of discharge plans.
So, bearing in mind the above – just some of the points raised in LPFT Trust Policy:
- Trust Policy clearly states right to privacy and dignity and yesterday’s visit and that of the 18th was far from dignified and most certainly upsetting for Elizabeth.
- What exactly are the concerns on behalf of Dr Khokhar who is clearly the person behind the restrictions as stated in Trust HQ letter?
- Is it not breach of privacy and dignity for Elizabeth to have 2 members of staff sitting in and listening to every word? Is this acceptable in terms of privacy and dignity? This does not seem to be in line with LPFT Policy.
- Is safeguarding going on again behind my back and at what stage is this at?
- Is DoLs in place and LPFT gone behind our backs to court to apply this under 6b MCA? Surely this cannot be the case when Elizabeth is already held under the MHA in which case the less restrictive practice should be made surely unless I have misread LPFT’s Policy in that respect. Please confirm?
- Finally within Equality Act and HRA 1998 it is clearly stated consideration as per below.
- Elizabeth made a valid point at the only ward round I was present – “why do members of staff push me up against a wall and inject me when I was doing nothing at the time?
- Public sector Equality Duty
The public sector Equality Duty came into force across Great Britain on 5 April 2011. It means that public bodies have to consider all individuals when carrying out their day-to-day work – in shaping policy, in delivering services and in relation to their own employees.
It also requires that public bodies have due regard to the need to:
- eliminate discrimination
- advance equality of opportunity
- foster good relations between different people when carrying out their activities
he Act sets out your human rights in a series of ‘Articles’. Each Article deals with a different right. These are all taken from the ECHR and are commonly known as ‘the Convention Rights’:
Hope the above is given consideration. After two years+ of incarceration and held on an ongoing indefinite section, when Elizabeth was released from Section 3 under Enfield she was living in the community peacefully, before we moved to Lincolnshire where I provided a small bungalow for her to live independently and bring her closer to rest of family. She had no care or support in the previous community Under S117 apart from the depot which she was compliant with. Why is she still held and treated like a restricted prisoner after all this length of time under LPFT?
Elizabeth should not be treated as though on DoLs when held under S3 MHA as this kind of treatment does not seem to be in line with your own Policy and would appear unlawful.
As somebody who has been responsible for records and H&S for many years and who has also seen at first hand NHS staff working towards accreditations I do not see any regard for Human Rights or the Equality Act or LPFT Policy.
I would like to know the reasons for this degrading, restrictive practise on the part of LPFT and how long will these restrictions of 2-1 supervision be in place for?
Yours sincerely
Susan Bevis
Mother and POA
TEAMS MEETING 01.11.2023
Unfortunately technical problems my end so I could only write my comments but at least my comments are recorded to all attending on the massive list above. No-one else from the family on that list and many strangers. I could see and hear what they were saying at least. Former Area of Enfield care coordinator Hannah Kajue well known to us as a family was present. They are responsible for S117 which was something I was not aware of prior to moving. Only depot injection provided- no care or support whatsoever.
My first question was about the restrictions which are of course against Elizabeth’s wishes and human rights.
Dr Waqqas Khokhar who is the Responsible Clinician of Castle Ward, PHU Lincolnshire County Hospital (LPFT) said that the restrictions would continue on me visiting my daughter – he had already mentioned about concerns regarding me being a “bad influence” on Elizabeth. However Elizabeth has full capacity as far as we are concerned and wants to come home. Because of three in house capacity assessments all flawed a whole team are deciding what they think is best interest on behalf of my daughter. Surely nothing should ever be done in-house and during a meeting before Sharon Harvey Director of Nursing and Quality LPFT it was verbally offered another completely independent capacity assessment but what about those done by the CoP at the same time? I have already heard the result of one of them that did not show Elizabeth to have no capacity. It is disgraceful that this LPFT are going along with the flawed capacity assessments to decide on their OWN intentions together with former area of Enfield involved. I believe they are also doing safeguarding once again behind my back.
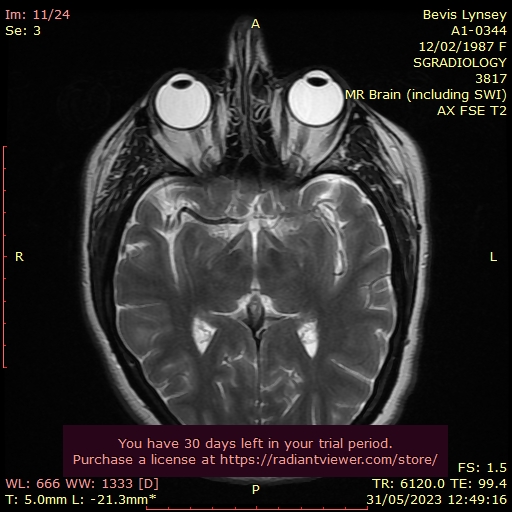
The safeguarding should be solely done on LINCOLNSHIRE PARTNERSHIP TRUST RATED GOOD BY THE CQC. That is because we are all now aware of the serious accident at Ash Villa where Elizabeth banged her head badly on the floor of the seclusion room. Since then she has been suffering from what looks like fits. All her existing appointments were cancelled as unnecessary by LPFT who were happy to rely on scans going back to 2015 stating “NORMAL”.
Dr Khokhar mentioned about the EEG that everything was normal however none of this is of any consolation now Elizabeth has these frequent episodes since Ash Villa.
Dr Khokhar mentioned about another MRI scan which THEY LPFT would arrange. However I told him that a private scan had already been done and was with other experts. I also told him that these scans had been sent to the Consultant Neurologist directly based by another team under Lincolnshire. Hopefully another team concerned with physical health expertise under neurology will look into all the abnormalities seen on the MRI scan.
All I have ever wanted was for my daughter to be listened to and to have fair treatment. This has not been the case under LPFT where no laws are abided by and they are even in breach of their own code of conduct and Policy. Her physical health has been totally ignored reliant on a previous scan in 2015 and ignoring all the other scans that showed abnormality on the discharge note.
The Ombudsman too need to look into everything as a vulnerable person’s life and wellbeing is at stake here.
The CQC need to look into how many times my daughter is being frequently rapidly tranquilised and she is being forced to take Procyclidine. She is being deprived family visiting rights and leave after over two years. There has been abuse of power and process.
Elizabeth has requested another doctor because this particular doctor will not listen and you can barely get a word in edgeways. Dr Khokhar said this would not be facilitated as there was noone to act as such however now things have changed in terms of appointment which I will quote later.
Promises given by Directors of Nursing for LPFT (Sharon Harvey) and the ICB (Martin Fahey) was a CTR (Community Treatment Review) – originally denied but was promised that the CTR would be independently chaired like in Enfield where the independent chair said “the whole thing stinks”. Yes it most certainly does when a vulnerable person is not getting the correct care and denied human rights to see their family.
The other matter that was briefly discussed was the displacement of yet another NR appointed in my place but this NR has recovered now from illness and it is clearly a conflict of interest to appoint the LA who have failed in every way to do their job in safeguarding under the role of NR for so long. She was living in squalid conditions and on a faulty bed, so many health and safety issues plus under what would appear a DoLs yet nothing properly set up as I checked. Treated like a restricted prisoner, denied S17 leave and constantly injected to the point other patients complained. Appalling treatment of a vulnerable person and family.
I would like a FULL ENQUIRY by the CQC into the conduct of the MHA office under Ash Villa and to date what is going on behind my back under safeguarding once again. If they are using safeguarding to protect themselves because I have found out about the accident and injury to my daughter and so have other family members then this needs proper examination as to where concerns lie. As mother and POA I have a duty to speak up against such cover-ups when certain trusted professionals do not go by their own code of conduct and breach of Trust Policy and MHA and MCA re the 3 flawed capacity assessments.
WWW.LPFT.NHS.UK
THE RESPONSIBLE CLINICIAN
The functions of the RC are no longer restricted to medical practitioners.
It may be undertaken by practitioners from other professions, comprising nursing, psychology,
occupational therapy and social work, this by virtue of the fact that Directions specify.
The professions whose members may be approved and the type of skill and experience required have been set out in the Mental Health Act 1983 Approved Clinician Directions 2008 are:
a registered medical practitioner
· or a chartered psychologist
· or a first level nurse whose field of practice is mental health or learning
disabilities nursing
· or an occupational therapist
· or a registered social worker.
Approval under the Directions also requires an individual to demonstrate a comprehensive understanding of the role of the AC, the role of the RC, legal responsibilities and key functions.
The categories of competencies required include:
· role of the approved clinician
· assessment
· leadership and multi disciplinary team working
· care planning
· treatment
· equality and cultural diversity
· mental health legislation and policy
· communication
Appointment of the responsible clinician
Where a patient becomes subject to compulsion, the hospital managers have a
responsibility to ensure that the patient is allocated an appropriate RC. [see Chapter 11of the Code]
The hospital managers must ensure that the RC for each patient is clearly identified.
Other ACs who are involved in the delivery of aspects of the patient’s care should also be clearly identified
The day to day responsibility for appointing or changing the RC will normally be
delegated to staff or other officers of the hospital. Nevertheless, overall accountability will remain with the hospital managers.
The decisions on who to appoint as the RC will be based on the individual needs of the patient concerned.
It is also possible that a patient may request for an alternative RC to be appointed. Where this is appropriate or practical, such a request may be accommodated. This has been denied to Elizabeth as Dr Khokhar refuses to step down and Elizabeth has said this in front of him too.
Approved Clinicians and Responsible Clinicians Workbook
Version 1 11 They arrange and co-ordinate the assessment, taking into account all factors to determine if detention in hospital is the best option for a patient or if there is a less restrictive alternative.
Point to note
A registered medical practitioner is specifically prohibited from being approved to act as an AMHP. This means that there will be a mix of professional perspectives at the point in time when a decision is being made regarding a patient’s detention.
This does not prevent all those involved from being employed by the NHS, but the skills and training required of AMHPs are intended to ensure that they provide an
independent social perspective.
Part 2 – Compulsory Treatment
· Section 20(3) – (5) Review of detention for treatment
The duty of the RC to examine a patient who is compulsorily detained for treatment within the two months before the period of detention expires, to determine whether they continue to meet the criteria for detention. If the criteria are met and the RC considers that it is appropriate to renew the detention, the RC must make a report to the hospital managers , in order that the period of detention will be renewed.
Before making their report the RC has a duty to consult at least one other person
who has been professionally concerned with the patient’s medical treatment and
who belongs to a profession other than that of the RC and that person has
confirmed in writing that he or she agrees that the grounds are met.
Section 17(1) – (4) Leave of absence from hospital
The RC may grant leave to be absent from the hospital to a patient who is
compulsorily detained, subject to such conditions (if any) as are considered
necessary in the interests of the patient or for the protection of other persons. She is of no risk to others.
Section 23 – Discharge of patients
The RC may make an order in writing discharging a patient absolutely from
detention, community treatment or guardianship.
Approved Clinicians and Responsible Clinicians Workbook
You will be aware that certain treatments require a second opinion (either as well as or in place of the patient’s consent) and that in some circumstances treatment can be
imposed without the patient’s consent.
In all these situations, the AC or other person in charge of the treatment now has the
functions previously held by the RMO. A typical example of this would be signing a
certificate to say that a patient is capable and willing to consent to the treatment.
An AC can visit and examine the patient for the purposes of a reference or application to the Tribunal under those provisions. It is no longer necessary for this duty to be performed by a registered medical practitioner.
In all cases the RC will be the AC with overall responsibility for the patient’s case. This is set out in section 34(1) of the 1983 Act.
ONGOING DETENTION
The RC who is assessing has a statutory duty to consult with one or more
professionals who have been involved with the patient’s medical treatment. Before
furnishing a renewal report, the RC must secure the written agreement of one such
professional.
The professional(s) consulted in this way must be members of a different professional grouping from that to which the RC belongs.
In addition, it would be good practice, wherever possible, for the RC to consult with
others who have been involved with the patient’s care. This could include members of the statutory, voluntary or independent services. However, there is no specific duty to do so.
Criteria on which Elizabeth’s continued detention would be judged are essentially the
same as those that had to be satisfied before she became subject to compulsory
measures in the first place.
These are that:
· She is suffering from a mental disorder of a nature or degree which makes it
appropriate for her to receive medical treatment in hospital, and physical Now that is in doubt. Medical treatment might have to be of a different kind following the private MRI scans the MH department did not want her to have.
· It is necessary for her own health or safety or for the protection of other persons that she should receive such treatment and it cannot be provided unless she is detained, and not met The only risk is towards my daughter who has been denied MRI scan and Neurologist appointments already arranged by Enfield leaving me to pay for this myself privately.
· Appropriate medical treatment is available for her. Not met – totally wrong what they are doing.
If Elizabeth is to continue to be detained for treatment under section 3, the RC must be
satisfied that all three of the above criteria are met.
All clinically recognised mental illnesses such as schizophrenia, bipolar disorder,
anxiety or depression would fall under this definition. So too would personality
disorders, eating disorders, and autistic spectrum disorders. I do not see Cavernomas, epilepsy and tumours listed
The purpose of medical treatment is to “alleviate or prevent a worsening of the disorder or one or more of its symptoms” (section 145). They are making her worse re her physical health than ever. She has an injury.
In Elizabeth’s case, her diagnosis is in severe dispute. Pathological tests have been denied under LPFT for over 2 years now and it is only now she has been referred to a Neurologist under Lincolnshire United Partnership Trust – that deals with primary care and thank goodness for that.
treatment for her. The fact that this treatment is currently unavailable in Elizabeth’s local
psychiatric hospital does not necessarily mean that she cannot be detained there,
provided that an appropriate alternative treatment is available at this hospital. Then this is all wrong as there is no alternative treatment of a physical kind and how many more people in this position?
The second of the criteria for detention is that “it is necessary for their own health or
safety or for the protection of other persons that he or she should receive such
treatment”. Again if the diagnosis is completely different to mental illness and is of a physical nature a different kind of treatment clearly needs to be given. Why is that so unreasonable to ask for as a caring relative and why cant the NHS offer that especially when one of Elizabeth’s Doctor’s – Dr Shahpasandy did research on the Limbic System and found that a different kind of treatment worked to deal with the inflammation of the brain. Elizabeth also has a sebaceous cyst they say is benign but it is NOT BENIGN and they are just leaving it. Elizabeth should be entitled to have a family member with them if she is being taken for any surgery or appointments. When staff fail to get a patient under the MRI scanner I had no problems and therefore it is BEST INTEREST for the sake of physical health that carers are included and that is after all mentioned in LPFT Trust Policy.
If the RC is satisfied that the statutory grounds for continued detention are met, there is a statutory obligation for him/her to make a report to the hospital managers that this should happen, provided that he/she believes that this would be appropriate in all the circumstances of Elizabeth’s case. No idea who the Hospital Managers are but previously even when I was NR I was excluded from everything and Dr Shahpasandy said he was getting rid of me as NR. I had dared to ask for the research on my daughter that he was involved in when he found a patient did not have schizophrenia but inflammation of the brain and a different kind of treatment led to his recovery.
Thus, once the RC has come to a decision that continued detention is appropriate, a
report should be made on the appropriate statutory form which is used for this purpose.
This form is set out in Regulations. This will also require the written agreement of the
second professional whom the RC has been under a duty to consult. This written
agreement is provided on the statutory form.
How should the RC proceed if he/she comes to the conclusion that Elizabeth does
not meet the criteria for her detention to be continued?
If Elizabeth does not meet the criteria for continued detention, section 23(2)(a) of the Act
gives her RC the power to discharge her from detention.
This discharge served on the managers of the hospital in which Elizabeth has been detained. Note that, as always in respect of the Act, discharge refers to discharge from detention and does not refer to discharge from hospital.
Section 20 of the Act provides the legislative framework for all these actions, and the basic process for making this decision remains much as it was before.
The RC should also consult wherever possible with others who have been involved with the patient’s care, including the statutory, voluntary or independent services. Yes there have been plenty involved including Access Charity and NAS, private endocrinologist and neurologist
The value of involving carers and family in the decision making process is well
recognised because it provides a particular perspective of the patient’s circumstances and experiences. NO WAY HAS THIS EVER BEEN DONE.
The RC is, in fact, the only person who has the authority to renew the detention of a patient under section 3 of the 1983 Act. YES AND TO DENY FAMILY VISITING IN BREACH OF ART 8 HRA AND IN BREACH OF TRUST POLICY.
Definition of mental disorder:
The legislation now defines mental disorder as ‘any disorder or disability of the
mind’. This new definition provides a single, simple definition rather than specifying
categories of disorder. This is disturbing because the former RC Dr Shahpasandy did research into the Limbic system and with a different kind of treatment his patient recovered. Pathological tests are denied to patients under MH so underlying physical health conditions are simply covered up and that patient is not getting the right treatment. Notably Dr Shahpasandy’s patient got better when taken off the same drug that Elizabeth was on and if someone has inflammation of the brain then they need anti-inflammatory drugs surely. The other reason I am being denied contact with my daughter is that Rapid Tranquilisations are given frequently and often without any reason. No correct procedures are being carried out before the injection is given. Absolutely appalling! I have requested under FOI lPFT RT log and Policy which I am still waiting for.
Grounds for detention:
If patients are to be detained for treatment under section 3 and related sections of
Part 3 there is an important addition to the criteria that ‘appropriate medical How inappropriate is it for a vulnerable patient to have frequent rapid tranquilisations and even be forced to take Procyclydine which is not part of the treatment. It is affecting Elizbeth’s eyesight and walking ability they are desperately trying to play down.
treatment’ is available for the patient. As a result, it will not be possible for patients to be compulsorily detained or their detention renewed unless medical treatment is available for them which is appropriate taking into account the nature and degree of their mental disorder and all the other circumstances of their case. The previously used ‘treatability test’ (as it was called) has now been abolished.
Disabilities of the brain would not be classified as mental disorders unless they give rise to a disability or disorder of the mind as well. The extent of injury they are treating as a mental disorder needs further examination by experts in the field of Neurology only.
Treatability test required the decision-makers to determine whether medical
treatment was ‘likely to alleviate or prevent deterioration in the patient’s condition’. This requirement no longer applies. If someone has epilepsy are they physically restrained and injected whilst having a fit. Why on earth is this being done under MH?
“’Medical treatment’ includes nursing, psychological intervention and specialist mentalhealth habilitation, rehabilitation and care”. [section 145 of the Act]
Purpose of treatment
The Act also stipulates that the purpose of medical treatment “is to alleviate, or prevent a worsening of, the disorder or one or more of its symptoms or manifestations”. A ‘disorder’ when in fact an injury that needs further investigation????? Why were we not informed of the accident??
Point to note
An important factor here is that this is about the purpose of the treatment, rather than
being about its likely outcome (as was the case in the previous ‘treatability’ test).
Point to note
The overall effect then is that these conditions cannot be met unless medical treatment:
· is available to the patient in question
· is appropriate IT CLEARLY IS NOT APPROPRIATE WHAT THEY ARE DOING AND AGAINST THE LAW.
· takes account of the nature and degree of the patient’s mental disorder, and
· takes account of all other circumstances of the case.
The Mental Health Act 1983 sets out the legal framework that underpins the detention and treatment of patients under compulsion. THE MENTAL HEALTH ACT IS NOT FIT FOR PURPOSE AND FAILING TO PROTECT THE VULNERABLE PATIENTS HELD ON NEVER ENDING SECTIONS DEPRIVED OF PATHOLOGICAL TESTS SUCH AS NEUROLOGY/MRI
The Mental Health Act 1983 Code of Practice provides guidance, including
good practice, as to how the Act should be applied. It also sets out principles which
should inform decisions under the Act.
The Code of Practice highlights, where relevant, the connections between the 1983 Act and other legislation, such as the Mental Capacity Act 2005.
The 1983 Act provides that practitioners must have regard to the Code in relation to
admitting persons to hospital or guardianship, community patients and in providing
medical treatment to patients.
Failure to do so could give rise to legal challenge. A court, in reviewing any departures from the Code, will scrutinise the reasons for the divergence to ensure there is sufficient and convincing justification in such circumstances. Nothing against medical treatment following full investigation by the Consultant Neurologist. The scans are with the Consultant Neurologist and several other experts as all I want is for my daughter to be treated fairly and correctly.
To put it simply, the Code of Practice is designed to guide practitioners in discharging their powers and duties under the 1983 Act. It provides practical guidance on all aspects of such matters.
Chapter 1 of the Code of Practice provides a set of nine guiding principles which should be considered whenever a decision has to be made about a course of action under the Act. The principles work together to form a balanced set of considerations which should inform all decision-making
Chapter 14 of the Code emphasises the importance of a holistic approach to providing care and treatment, and of involving users and carers in creating and reviewing the care plan. It also sets out that those who should be involved in preparing the care plan to meet the patient’s needs include: Holistic approach – this is laughable as her medication raised to enormous levels.
– the patient, if he or she wishes and/or a nominated
– the patient’s responsible clinician
– the patient’s care coordinator
– the patient’s carer (where they will be providing care that is identified in the care plan)
– members of the inpatient care team (if the patient is in hospital).
Chapter 4 of the Code makes it clear that the test requires a judgement about whether, in all the circumstances, medical treatment is available to the patient which is appropriate. This needs consideration of the nature and degree of the patient’s mental disorder and all other circumstances of the patient’s case. These other circumstance might, for example, include the patient’s physical health – how it might impact on the effectiveness of the available medical treatment for mental disorder and the impact that treatment might have in return:
· any physical difficulties that the patient has
· the patient’s culture and ethnicity
· the patient’s age
· the patient’s gender, gender-identity and sexual orientation
· the location of the available treatment
The treatment to be offered must be an appropriate response to the patient’s condition and situation.
But that needs to be properly determined by an expert in the field of Neurology.
RCs cannot grant leave of absence under section 17 for part 2 or unrestricted part 3
patients for longer than 7 consecutive days without first considering whether the patient should be discharged onto SCT. In effect, RCs will have to demonstrate that SCT has been considered and show why section 17 was more appropriate. No S17 granted and visits highly restricted – breach of Art 8 HRA
DEPRIVATION OF LIBERTY NOTES
Deprivation or restriction of a person’s liberty
The principal question that is likely to concern you in your role is whether a particular
set of circumstances amounts to actual deprivation of someone’s liberty or whether it is a restriction of liberty.
The European Court of Human Rights has said that the difference between restriction and deprivation of liberty is one of degree or intensity rather than of nature or substance.
To determine whether a person is being deprived of liberty, there must be an
assessment of the specific factors in each individual case. Every case must be
assessed on its own terms, and every possible instance has to be taken on a ‘case by case’ basis.
Based on existing case law, the following factors might well be considered by the courts to be relevant when considering whether or not deprivation of liberty is occurring:
· The person is not allowed to leave the facility Yes
- The person has no, or very limited, choice about their life within the care home or Hospital Yes
- The person is prevented from maintaining contact with the world outside the care Yes
Standard authorisations Requesting authorisation
The managing authority must request authorisation from the supervisory body for a
person to be detained as a resident in a hospital or care home in circumstances which amount to deprivation of their liberty.
Qualifying requirements
Before a managing authority applies to the supervisory body for a standard
authorisation to detain a person as a resident in a hospital or care home in
circumstances which amount to deprivation of their liberty, it must be satisfied that the individual appears to meet the qualifying requirements.
There are six qualifying requirements against which the case will be assessed by the supervisory body:
1. age requirement
– the person must be aged 18 or over.
2. mental health requirement
– the person must be suffering from a mental disorder within the meaning of the
1983 Act.
3. mental capacity requirement 3 completely flawed assessments so they can take control – total abuse
– the person must lack capacity to decide whether or not they should be a
resident in the hospital or care home.
4. best interests requirement should be abolished and any assessments done independently.
– the deprivation of liberty authorised must be in the best interests of the person. in their own interests without consideration to anyone else in the family.
5. eligibility requirement
– a person is ineligible if they are already actually detained in hospital under the
1983 Act, or if they are on leave of absence from such detention or subject to
guardianship, SCT or conditional discharge and in connection with that are
subject to a measure which would be inconsistent with the authorisation if
granted.
6. no refusals requirement
– if there is a conflict, with another existing authority for decision-making for the
person, a standard authorisation for deprivation of liberty may not be given.
Urgent Authorisations
The managing authority can itself give an urgent authorisation for deprivation of liberty where it:
· is required to make a request to the supervisory body for a standard
authorisation, but believes that the need for a person to be deprived of liberty is
so urgent that it is appropriate to begin the deprivation before the request is
made, or
· has made a request for a standard authorisation but believes that the need for a
person to be deprived of liberty has now become so urgent that it is appropriate
to begin the deprivation before the request is dealt with by the supervisory body.
This means that an urgent authorisation can never be issued without a request for a
standard authorisation being made.
An urgent authorisation can only last for a maximum of 7 days unless in exceptional
circumstances it is extended to 14 days by the supervisory body.
CONCLUSION
“THE WHOLE THING STINKS!” SO MANY VULNERABLE PEOPLE BEING ABUSED BY A SYSTEM NOT FIT FOR PURPOSE AND IT IS NOT JUST LPFT OR BEHMHTNHS THIS IS NHS CARE AT ITS WORST THAT ALLOWS SYSTEMATIC ABUSE OF THE WEAK AND VULNERABLE AND SOMETHING NEEDS TO BE DONE ABOUT IT AND THE PEOPLE WHO NEED TO BE INVOLVED IN CHANGING THE MHA ARE NONE OTHER THAN THE PATIENTS AND CARERS THEMSELVES.