Evidence of New / Escalating Criticism of Lincolnshire Adult Social Care
Ombudsman / Care Act Failures
A recent (April 2025) LGO decision (ref 24-003-962) found fault in how LCC (via Lincolnshire Partnership NHS Trust, acting for LCC) handled a Care Act assessment and care plan for a person with mental and physical health needs. Specifically: no advocate was involved despite communication difficulties, care was inconsistent, and there was poor communication / information-sharing — this caused distress. Local Government Ombudsman
Another case (Centre for Adults’ Social Care report, June 2025) describes a woman with complex mental health needs whose move into the county triggered fragmented / inadequate support. LCC (via its partner trust) failed to provide consistent care, arranging too few hours vs her assessed need, and she suffered distress, hospital admissions, and isolation. cascaidr.org.uk
A separate Ombudsman ruling (July 2025) relates to transition from children’s to adult services. LCC made “errors in care package decisions and communications” for a young adult with disabilities (including transport for day-centre attendance), causing her to miss care. cascaidr.org.uk+1
Healthwatch Lincolnshire Feedback
The Healthwatch Lincolnshire report (2025) includes a case (Feb 2025) of an adult social care user whose health needs were compromised because of lack of proper care provision. According to the report, the person is a wheelchair user and needs increased care post-operation, but LCC could not guarantee provision for that increased care, leading to the cancellation of a surgery. Healthwatch Data
While this is not explicitly “mental health care,” it shows stress / risk in how adult social care assesses and responds to changing care-need demands — including when health interventions (surgery) would make care needs temporarily more intense.
Local Media / Policy
Lincolnshire World reported very recently (Oct 2025) that LCC officials are considering reducing the number of “active recovery beds” (mental-health-related step-down beds) from 29 to 24. That’s a significant signal: reducing capacity in part of the mental health recovery system could be seen as cutting back or deprioritising mental health care for adults. LincolnshireWorld
Complaint Statistics
In its 2024–2025 complaints report, LCC notes that 23 complaints from that year were escalated to the LGSCO about adult care. Lincolnshire County Council
While not all these will be about mental health, it suggests a non-trivial volume of serious complaints in the adult care sphere.
Interpretation & Assessment
The Ombudsman findings are the strongest concrete evidence: there are real cases where LCC has failed to provide or plan care properly for people with mental health or complex needs. These are not isolated paperwork mistakes, they have caused distress and had a material negative impact.
The Healthwatch case indicates that some people struggle to get social care to respond when their health needs (which may interact with mental health) change. That could suggest capacity / resource problems in LCC’s adult social care provision.
The proposal to reduce active recovery beds is worrying: if implemented, it could worsen recovery pathways for people needing step-down mental health care. That could be a policy direction that reduces service rather than expands it.
However, the CQC’s most recent (pilot) assessment of LCC adult social care is still “Good”, which means from a regulator’s perspective, the overall adult social care system is functioning reasonably well (though not without room for improvement, especially in certain pathways). Lincolnshire County Council+2Care Quality Commission+2
There is new and escalating criticism of LCC’s mental-health-related adult care: through Ombudsman decisions, Healthwatch reports, and potentially in policy (bed reductions).
The criticisms are not wholesale systemic collapse, but they do raise serious concerns about how well LCC is meeting the needs of vulnerable adults — particularly those with complex mental health or changing care needs.
Some of the key pressure points: assessment and care planning, continuity / consistency of care, capacity in recovery services, and responsiveness to changing needs.
Briefing Summary: Criticisms of LCC Adult Mental Health Care (2023–2025)
1. Financial & Demand Pressures
LCC’s 2024/25 financial performance review reports a significant overspend in mental health adult care:
Community supported living (for working-age / mental health clients) overspent by £3.2 million, of which £1,060,000 relates to “Growth in demand for DoLS / LPS” (Liberty Protection Safeguards) due to a much higher-than-expected increase in client numbers (94 new clients vs 25) planned). lincolnshire.moderngov.co.uk+2lincolnshire.moderngov.co.uk+2
Long-term residential mental health care also saw growth: 27 new clients, resulting in a £0.408 million overspend. lincolnshire.moderngov.co.uk+1
Short-term care (mental health) clients exceeded budgeted numbers, adding further financial pressure. lincolnshire.moderngov.co.uk+1
The budget for 2025/26 continues to forecast rising demand in mental health: LCC recognizes a 3–6% annual growth in working-age / mental health service demand. lincolnshire.moderngov.co.uk
In its executive meeting (Aug 2025), the Overview & Scrutiny Management Board flagged this as a “volatile and risk-based” budget area, with ongoing close monitoring. lincolnshire.moderngov.co.uk
Implication: LCC may be under-estimating both the scale and pace of demand growth for mental health care, risking repeated overspends and service strain.
2. Service Reduction Controversies – Active Recovery Beds
Local media (LincolnshireWorld) report that LCC is proposing to reduce the number of Active Recovery Beds (ARBs) from 29 to 24. LincolnshireWorld
These beds are used for people stepping down from hospital but not yet ready to return home, reducing them could limit “step-down” capacity. LincsOnline+1
The Council argues the reduction aligns with “presenting demand” and will improve occupancy (from ~70% to ~90%). LincolnshireWorld
However, some councillors have expressed concern: e.g., whether this reduction under-provides in the face of broader NHS / social care pressures. LincolnshireWorld+1
Implication: The proposed cut could undermine recovery capacity; critics worry demand may outstrip reduced supply, especially as patients leave hospital.
Ombudsman Findings – Assessment & Care Planning Failures
In LGO decision 24-003-962 (April 2025), the Ombudsman upheld a complaint against LCC:
LCC (via its partner, Lincolnshire Partnership NHS Trust) failed to provide reasonable adjustments in a Care Act assessment despite the complainant’s mental and physical health issues. Local Government Ombudsman
The decision-making was inconsistent: carers were not familiar with her, there was inadequate handover, and no advocate was involved even when needed. Local Government Ombudsman
The Council also made housing decisions (moving the person) that the Ombudsman found unsuitable. Local Government Ombudsman As a remedy: LCC must apologise and pay a sum to acknowledge the injustice caused. Local Government Ombudsman
A separate Cascaidr analysis (July 2025) highlights another case: LCC failed to properly manage a care package for a person with mental health and possibly autistic traits. Adult Social Care Centre
The complaint noted that LCC did not properly assess the person’s capacity or share information with providers, leaving her without adequate support. Adult Social Care Centre
The analysis argues that LCC’s assessment systems / legal understanding may be weak in dealing with complex, capacity-fluctuating mental health cases. Adult Social Care Centre
Another Cascaidr / Ombudsman case (Sept 2025): poor management of transition from children’s to adult services for a young woman with disabilities (including mental health / supportive needs). Adult Social Care Centre
The Council initially promised transport + day-centre attendance but later withdrew transport without confirming that a closer centre could meet her needs, resulting in missed care. Adult Social Care Centre
The Ombudsman found LCC at fault: decisions were made without fully checking alternatives; communication was confusing; and there was procedural failure in its authorisation processes. Adult Social Care Centre
The Council was required to apologise and pay a symbolic amount, and to remind staff about proper internal authorisation procedures. Adult Social Care Centre
Implication: There appear to be systemic weaknesses in LCC’s assessment, planning, and communication processes especially for people with complex mental health needs or transitioning from children’s services. This raises risk of unmet need, distress, and legal non-compliance.
Local Advocacy / Healthwatch Voice
Healthwatch Lincolnshire’s 2024/25 Annual Report shows increasing engagement, but also highlights challenges: while not all issues are mental health–specific, many concern social care access, capacity, and unmet needs. healthwatchlincolnshire.co.uk
In the 2024–25 interim work plan, Healthwatch identified “influencing decision-makers” and “addressing underrepresented groups” as key priorities, suggesting they are pushing for more responsive, inclusive care provision. healthwatchlincolnshire.co.uk
Local media commentary (LincolnshireWorld) also notes LCC acknowledging rising complexity in mental health care packages and growing costs:
“a major contributor to cost pressures … an increase in demand and complexity of mental health services.” LincolnshireWorld
Implication: Local citizen-led organisations are raising the alarm about escalating demand, growing complexity, and pressures on mental health adult care — suggesting these are not just financial issues but affect quality and accessibility.
Strategic & Systemic Risks
During a Council Executive meeting (July 2025), a councillor (Steve Clegg) explicitly questioned LCC’s mental health community support overspend. The Executive Director (Adult Care) acknowledged demand is rising “faster than elsewhere” and hinted at concerns over the quality of existing service delivery. Open Council Network
LCC’s written evidence to Parliament (recent submission) also warns that demand for adult mental health care is exceeding previous forecasts, putting “increasingly strained” pressure on the system. UK Parliament Committees
Implication: The financial and service pressures are not short-term or one-off: there’s a real risk that demand continues to outpace LCC’s capacity, potentially degrading care quality or forcing tough decisions (like bed cuts).
Overall Summary
Demand is rising fast: LCC is seeing more working-age / mental health adult clients than budgeted for, driving large cost overruns.
Service capacity is under threat: Proposed reductions in Active Recovery Beds raise concerns about recovery pathways.
Professional standards are being questioned: Ombudsman decisions show LCC sometimes fails in assessments, support planning, and legal duties, especially for those with complex, fluctuating mental health needs.
Local voices (Healthwatch, Councillors) are pushing back: There is growing unease about how LCC is managing this demand, both financially and in terms of service delivery.
Strategic risk is real: Unless LCC adapts, by increasing capacity, improving assessment processes, and planning strategically — there is a danger that its mental health adult care provision will become unsustainable.
A separate Cascaidr analysis (July 2025) highlights another case: LCC failed to properly manage a care package for a person with mental health and possibly autistic traits. Adult Social Care Centre
The complaint noted that LCC did not properly assess the person’s capacity or share information with providers, leaving her without adequate support. Adult Social Care Centre
The analysis argues that LCC’s assessment systems / legal understanding may be weak in dealing with complex, capacity‑fluctuating mental health cases. Adult Social Care Centre
The Care Act 2014 requires councils to assess any adult who appears to need care and support, regardless of financial circumstances, and to involve the individual and any carer or anyone else they wish to be involved. Assessments must be timely, involve the person, and consider their wellbeing and desired outcomes. Care and support plans must be co-produced, include a personal budget, and be responsive to changing needs.
When a person moves between council areas, there are statutory duties to ensure continuity of care (section 37), but they do depend on the destination council knowing that the person is on their way.
Councils must also consider reasonable adjustments for communication and mental health needs, and ensure advocacy is provided where it is triggered by the concept of the person’s substantial difficulty engaging in the Care Act processes of assessment, care planning or revision (regardless of having a willing relative) without one being appointed.
The failure to provide adequate care and support, or to arrange advocacy, is a breach of statutory duty. It renders the assessment invalid, in community care and public law and that has been the case since the Haringey judgment in 2015.
A delayed discharge case is when a patient is medically ready to leave a hospital but remains there for non-medical reasons. The delay can be caused by factors like a lack of available social care, insufficient community care packages, or issues with the hospital’s own processes. These delays are a major concern as they reduce hospital bed capacity, potentially leading to poorer patient outcomes and increased healthcare costs.
Delayed discharges: why it’s hard to say how many are due to social care capacity
Here’s a multiple-choice quiz. What percentage of delayed discharges from hospital are caused by lack of adult social care capacity? Is it:
a) Most of them
b) 50%
c) 12%
d) There’s no way of knowing for certain.
The answer is d): we just don’t know. You get half a point if you said c) because 12% is the most we can definitely attribute to lack of social care capacity from the publicly available data. However, you’d be forgiven for thinking it was b) or even a) if you simply read the media coverage. In December, the Royal College of Nursing was quoted as saying that there was ‘barely a spare bed’ left in NHS hospitals due to a lack of capacity in social care; while in January, the NHS Confederation was reported as saying that 20% of NHS bed capacity was taken up by patients who were only there because they ‘cannot get a suitable care package’.
“Yet we don’t know the number – because, with the best of intentions, we chose to stop asking.”
Yet we don’t know the number – because, with the best of intentions, we chose to stop asking. In 2020, NHS England stopped separating out reasons for delay between health and social care. The reasoning, based on discussions with health and care organisations, was that delays were often complex, and instead of allocating them to one or other partner, systems should take responsibility, rather than individual sectors.
The most recent data recording, introduced in May 2024, requires discharge hubs (or sometimes wards) to classify the causes of delay into one of five categories:
Hospital process (issues within the hospital’s control, such as medication or transport)
Wellbeing concerns (issues outside the hospital’s control, for example where a family has doubts about a patient’s readiness for discharge)
Care transfer hub process (most commonly where the patient’s destination has not yet been decided)
Interface process (typically where transfer plans are underway but have not yet been completed)
Capacity (where the service needed by the patient is not yet available).
Except for hospital process, all these categories include delays that are due to both the NHS and social care. For patients with stays of at least 14 days (the only publicly available measure), on average 9,309 people were delayed each day in March 2025. Of these, 3,203 delays were ascribed to ‘capacity’, followed by interface process (2,639), hospital process (1,754), care transfer hub process (1,200) and wellbeing concerns (514).
If we focus on those 3,203 capacity delays – because lack of social care capacity is often cited as a key cause of delayed discharges – the single largest reason (966 people delayed) is lack of ‘bed-based rehabilitation, reablement or recovery services’.
This covers a wide range of health and care services, some of which are commissioned by NHS trusts, some by local authorities and some jointly. Even discharge hubs would not be able to allocate them to ‘the NHS’ or ‘social care’. The same applies to ‘home-based rehabilitation, reablement or recovery services’ (502 people delayed), which again cannot be split neatly into social care or NHS.
In fact, only three of the sub-categories – lack of home-based social care services (257), lack of residential or nursing care (762), and people waiting for restart of existing social care services (63) – are solely attributable to social care. But these account for only 34% (1,082) of the 3,203 total ‘capacity’ delays and only 12% of the total 9,309 delayed patients. The real figure for social care delays will be higher because it will include some of the bed-based and home-based rehabilitation and reablement delays but is not counted.
“Yet the NHS and social care are two distinct systems, funded differently, usually commissioned differently and often with different immediate concerns.”
Author:
Into that data vacuum has emerged a range of guesses and estimates, some more authoritative than others. For example, in March NHS England told the House of Commons Health and Social Care Committee that around a fifth of bed days (note that this is a different measure to the publicly available one) lost to delayed discharge ‘are for individuals accessing adult social care packages on discharge’.
In an ideal world, it might not matter. Local systems would be working together to identify problems, avoiding blame and finding joint solutions. Perhaps most are already. Yet the NHS and social care are two distinct systems, funded differently, usually commissioned differently and often with different immediate concerns. On the NHS side, there is intense media and public concern about hospital capacity, A&E waits and ‘corridor care’. On the social care side, there is a longstanding grievance about lack of funding.
In these circumstances, it has sometimes suited both sides for lack of social care capacity to be seen as the key cause of hospital discharge delays. It allows social care to make the case for more money and deflects attention from the NHS causes of delay. This is why the headlines are tolerated, sometimes encouraged.
“It allows social care to make the case for more money and deflects attention from the NHS causes of delay. This is why the headlines are tolerated, sometimes encouraged. ”
Author:
Yet it can still rankle within social care if it is held largely responsible for a problem to which it is, in fact, only a minority contributor. There is a long and inglorious tradition of blaming social care for hospital discharge delays.
There is also irritation about the word ‘capacity’: there is plenty of capacity in care homes, says the sector (occupancy has still not quite returned to pre-pandemic level); the issue is that commissioners (in both the NHS and local authorities) are not sufficiently well organised and are unable or unwilling to pay a fair price for it.
In this difficult environment, avoiding a blame game on hospital discharge was always going to be ambitious. It’s proved to be that – and more. Time to accept reality and publish a credible official estimate of the respective responsibilities for delayed discharge of health and social care.
Held at:County Offices, Newland, Lincoln, LN1 1YL Extract from Minutes of the Adults and Community Wellbeing Scrutiny CommitteeLincolnshire County Council A meeting of the Adults and Community Wellbeing Scrutiny Committee took place on Wednesday, 4 September 2024 at 10.00 am in the Council Chamber, County Offices, Newland, Lincoln LN1 1YL. Debbie Barnes OBE Chief Executive.
The Minutes stated: “Many older adults may have been misdiagnosed with mental health issues for decades, often leading to a misunderstanding of their true cognitive and emotional needs. Data was being gathered on these individuals, especially those with learning disabilities, who tend to be identified earlier in their lives, allowing for potentially more effective interventions. However, despite this positive trend, there were significant challenges in the system????The Integrated Care Board (ICB) recognized the need for immediate action and funded various services for 16-18 year olds, aiming to create a streamlined pathway for young individuals needing support. Unfortunately, there is a national issue with excessively long waiting lists for neurodevelopmental services, which further complicated access to necessary care.Waiting times for diagnosis were reported to be up to a year (4 IN ELIZABETH’S CASE) locally for those seeking help; in some regions, it could extend to an alarming seven years elsewhere, exacerbating the situation and leaving many individuals without the support (AND CORRECT TREATMENT) they desperately needed. This stark discrepancy highlights not only the urgent need for improvements in service delivery but also the importance of re-evaluating how mental health and developmental disorders are diagnosed across different age groups.”
In Elizabeth’s case, Developmental was mentioned in the first instance and as far back as 2007 scans were not normal. Being denied pathological tests goes well beyond a year – over a lifetime combined with former area, well before moving but now detention under the MHA is in its fourth year and there should therefore be no excuses for any further delays for essential neurological tests. What is the point in a CTR that does not review treatment effectively, excluding physical health and family for a vulnerable person held long term under MH for following reasons:
When is Referral for Neurological Testing Necessary?
Referral for neurological testing may be clinically indicated in several situations, including but not limited to:
Neurological symptoms such as persistent headaches, dizziness, weakness, visual disturbances, or cognitive changes.
Manifestations of seizures or fits or neurological reactions to stimuli or potential allergens.
Red flag symptoms indicating serious underlying conditions like a brain tumour, stroke, or multiple sclerosis.
Unexplained neurological signs after an injury or trauma, particularly head injuries, where a clinician might suspect a neurological disorder.
If a responsible clinician fails to refer a patient when such symptoms or red flags are present, and that failure leads to harm (e.g., delayed diagnosis of a serious neurological condition), there may be grounds for a negligence claim.
A clinician might be at risk of a negligence claim if they fail to refer a patient for neurological testing when clinically indicated, especially if such a failure leads to harm that could have been avoided with appropriate testing and treatment.
It is every bit possible that Elizabeth has been subjected to many years of inappropriate treatment due to faulty diagnosis and huge amounts of endocrine disrupting drugs, not to mention many years deprivation of liberty that could have been avoided with a more thorough medical examination.
Case law, such as A v East of England Ambulance Service NHS Trust, emphasizes that clinical decisions must align with accepted medical practices. If a clinician’s actions are within the range of what a responsible body of medical professionals would consider reasonable, they are less likely to be found negligent. However, if their failure to refer deviates from such standards and causes harm, they could be held liable.
A v East of England Ambulance Service NHS Trust [2017] UKSC 19:
This case concerned whether a medical professional breached their duty by failing to appropriately investigate or respond to a patient’s symptoms. Although it was about a failure in emergency care, it emphasizes the importance of considering the duty to investigate symptoms properly and the risks of failing to do so. A clinician failing to refer a patient for neurological testing might be considered negligent if it can be shown that such an investigation was warranted by the patient’s presentation.
The Bolitho v City and Hackney Health Authority[1997] 3 WLR 1151 case is a key ruling in clinical negligence law, refining the Bolam test (from Bolam v Friern Hospital Management Committee [1957]).
Ruling in Bolitho:
In this case, the House of Lords considered whether a doctor was negligent for failing to attend a child in respiratory distress, despite being called to do so by nursing staff. The doctor’s absence allegedly led to the child’s death.
The central issue was whether the doctor’s decision not to attend could be justified by the standard of practice accepted by a responsible body of medical opinion (the Bolam test). In other words, was the failure to attend a reasonable decision, according to the practices of a responsible group of doctors?
The House of Lords held that the Bolam test is not an absolute shield for professionals. Although medical practice is determined by the opinion of a responsible body of medical professionals, this does not mean that any opinion, however unreasonable, will be accepted. Courts have a role in ensuring that the medical opinion is “logical and defensible”. In essence, the court can reject a medical opinion if it is deemed illogical or irrational.
Summary of the Key Points:
The Bolitho ruling clarifies that medical professionals’ practices must be reasonable and defensible. Courts will scrutinize the validity of medical opinions in negligence cases.
It made clear that even if a practice is accepted by a body of medical professionals, if that practice is not supported by a logical or reasonable explanation, it cannot be relied upon to defend against a negligence claim.
The decision to not attend the patient in Bolitho was deemed negligent because the medical practice relied upon did not have a logical basis.
So what is the ‘logical basis’ for not sending Elizabeth for tests when they are clearly needed?
The Bolitho decision thus refined the Bolam test, adding an element of judicial oversight to ensure medical opinions are reasonable and coherent, not merely accepted by a group of professionals.
Diagnostic error in mental health: a review Bradford A, et al. BMJ Qual Saf 2024;33:663–672. doi:10.1136/bmjqs-2023-016996
There is sufficient evidence here already to link the lesions and resultant inflammation with what they misdiagnose as schizophrenia and this is even evident in Elizabeth’s former doctor’ s work: Dr Shahpesandy.
It is scandalous that with the number of patients known to be misdiagnosed that there is not a root and branch re-examining of mental health assessments. It is not psychiatrists and AMPHs who should have exclusive domaine here. The examination is nowhere near complete without a thorough neurological and immunological/endocrinological examination. Our national mental health policy is entirely in the sway of psychiatrists and drug companies.
A failure in pathophysiological testing for organic contributions can significantly contribute to the prevalence of misdiagnosis in schizophrenia. Reports and studies have indicated that the prevalence of misdiagnosis in schizophrenia can be significant, with estimates often cited in the range of 10% to 40%, depending on the specific context, population, and research methodology.
Given the complexities of diagnosing schizophrenia, it is crucial for mental health professionals to use comprehensive assessment approaches to enhance diagnostic accuracy and reduce the likelihood of misdiagnosis.
Lack of Comprehensive Assessment:
Many clinicians do not conduct thorough pathophysiological assessments, such as neurological evaluations and laboratory tests, which can lead to missing underlying medical conditions that mimic or contribute to psychiatric symptoms. Some clinicians over emphasise the subjective nature of psychotic disorders and actively discourage proper pathophysiological assessments.
Overlapping Symptoms:
Certain medical conditions (e.g., infections, autoimmune disorders, endocrine abnormalities) can present symptoms similar to those of schizophrenia. Without appropriate testing, these conditions may be misidentified as primary psychiatric disorders.
Neuroimaging and Biomarkers:
Advances in neuroimaging (like MRI or CT scans) and the discovery of potential biomarkers for various conditions are important for identifying organic contributions to psychosis. If these tools are not utilized, it can result in misdiagnosis.
Co-Occurring Disorders:
When an underlying medical condition is present alongside schizophrenia, it may complicate the clinical picture and lead to misunderstanding or misattribution of symptoms, resulting in a misdiagnosis.
Education and Awareness:
Clinicians may not always consider organic causes when diagnosing schizophrenia, especially if they lack training or awareness about how medical issues can manifest as psychiatric symptoms.
Stigma and Assumptions:
There may be an inclination to diagnose psychiatric conditions like schizophrenia without sufficiently exploring organic causes, particularly in patients with risk factors for mental illness, leading to overlooking potential medical diagnoses.
Case Reports:
Numerous case studies and reports highlight instances where patients initially diagnosed with schizophrenia were later found to have organic pathologies, emphasizing the necessity of pathophysiological testing in uncertain cases.
Inadequate pathophysiological testing increases the likelihood that clinicians may overlook organic contributions to a patient’s symptoms, leading to a higher prevalence of misdiagnosis of schizophrenia. Comprehensive evaluation approaches that integrate both psychiatric and medical assessments are essential for accurate diagnosis and effective treatment.
The misdiagnosis of schizophrenia can occur for several reasons, but the following are some of the main contributing factors:
Symptom Overlap:
Schizophrenia shares symptoms with various other mental health disorders, such as bipolar disorder, major depressive disorder, and personality disorders. This overlap can lead to confusion and misdiagnosis.
Incomplete Clinical History:
A thorough assessment requires a detailed clinical history, including past medical and psychiatric treatments. When this information is lacking or overlooked, it frequently leads to inaccuracies in diagnosis.
Subjective Assessment:
Psychiatric diagnoses often rely on subjective assessments of symptoms and behaviours. Variability in how clinicians interpret and diagnose these symptoms can result in inconsistencies and misdiagnosis.
Lack of Awareness or Training:
Some clinicians may not be adequately trained to recognize the nuances of schizophrenia or the range of conditions that can mimic its symptoms, leading to incorrect diagnoses.
Stigma and Assumptions:
Societal stigma surrounding mental illness may lead to hasty or biased conclusions, particularly in emergency settings where rapid assessments are made under stress.
Co-occurring Disorders:
Many individuals with schizophrenia may have co-occurring disorders (e.g., substance use disorders, anxiety disorders), complicating the clinical picture and leading to misdiagnosis.
Cultural Factors:
Cultural differences in the expression and interpretation of symptoms can affect diagnosis. Clinicians may misinterpret culturally specific symptoms as pathological.
Insufficient Diagnostic Tools:
While there are diagnostic criteria (like DSM-5 or ICD-10), there are no objective tests (e.g., blood tests or imaging) to confirm a schizophrenia diagnosis, leading to a over-reliance on observed behaviours and self-reported symptoms.
These factors highlight the need for comprehensive assessments and clinical awareness to reduce the rates of misdiagnosis in schizophrenia.
Failing to conduct thorough pathophysiological tests when diagnosing schizophrenia can have several significant serious consequences:
Misdiagnosis:
Schizophrenia shares symptoms with other mental health disorders such as bipolar disorder, depression, and schizoaffective disorder. Without comprehensive testing, there’s a risk of misdiagnosing the condition, leading to inappropriate treatment plans.
Inappropriate Treatment:
Inaccurate diagnosis can result in prescribing incorrect medications, which might not alleviate symptoms and could cause adverse side effects. Patients might also miss out on the benefits of effective therapeutic interventions tailored to their actual needs.
Delayed Treatment:
Insufficient testing might delay the correct diagnosis, postponing necessary interventions. Early and accurate diagnosis is crucial for effective treatment, and any delay can worsen prognosis and lead to more significant deterioration in quality of life.
Poor Prognosis:
Without targeted interventions, patients may experience worsened symptoms and a decline in functioning. More comprehensive evaluations can help identify specific needs and comorbid conditions, which are integral in planning effective management strategies.
Increased Healthcare Costs:
Misdiagnosis or delayed diagnosis can lead to increased healthcare costs due to unnecessary treatments, potential hospitalizations, and more extensive long-term care due to unmanaged symptoms.
Impact on Quality of Life:
The individual may suffer from ongoing symptoms that could affect their daily life, social relationships, and occupational functioning. Effective treatment hinges on an accurate diagnosis, allowing patients to manage symptoms and improve their overall quality of life.
CAVERNOMAS
A thorough diagnostic process, including pathophysiological tests are necessary and help ensure that patients receive the right diagnosis and appropriate treatment, improving outcomes and reducing the burden of the disease.
A cavernoma, which is a type of vascular malformation in the brain, can potentially interfere with neurotransmission and lead to symptoms that might be misinterpreted as psychosis. Cavernomas are clusters of abnormally formed blood vessels that can disrupt normal brain function by causing bleeding, inflammation, or other structural changes.
Cavernomas, especially in areas like the temporal lobe, can cause seizures. Seizures can sometimes present with confusion, disorientation, or altered perceptions, which could be mistaken for psychotic symptoms. For example, if the cavernoma causes focal seizures, these could manifest as hallucinations, paranoia, or delusions, which are all features of psychosis.
Cavernomas, depending on their location, can affect areas of the brain responsible for cognition and emotion regulation. If a cavernoma leads to functional changes in these regions, it could cause alterations in behaviour or mood, potentially resembling symptoms of a psychiatric disorder.
A cavernoma can disrupt the normal flow of neurotransmitters in the brain, especially if it causes local damage to nerve cells or interferes with blood supply. Neurotransmitter imbalances can contribute to mood swings, hallucinations, or altered perceptions, which may be mistaken for psychotic episodes.
In some cases, the physical stress and changes caused by a cavernoma, such as chronic headaches, seizures, or neurological deficits, can also lead to psychiatric symptoms, such as anxiety, depression, or even psychotic-like symptoms. These may be misdiagnosed as primary mental health issues.
Given these possibilities, a thorough neurological evaluation, including imaging studies like an MRI, is crucial for distinguishing between a primary psychiatric disorder and a neurological condition like a cavernoma. If psychosis-like symptoms are present, a neurologist or psychiatrist should look at a range of factors to rule out any underlying brain pathology, including vascular malformations like cavernomas.
The misdiagnosis of schizophrenia due to underlying brain lesions or cerebral inflammation is a known but relatively underreported phenomenon. Although schizophrenia is primarily considered a psychiatric disorder, its symptoms can overlap with neurological conditions that cause similar cognitive and behavioural disturbances, like brain lesions, inflammation, or other structural abnormalities.
Cerebral inflammation and brain lesions, such as those caused by vascular malformations (like cavernomas), brain tumours, endocrine disorders and autoimmune diseases, can lead to cognitive impairments, mood disturbances, hallucinations, or delusions, which are also hallmark symptoms of schizophrenia. When these neurological issues are undiagnosed, individuals may be misdiagnosed with a primary psychiatric condition like schizophrenia, especially if there’s a lack of awareness about the neurological possibility.
As for the estimated incidence of misdiagnosis, studies suggest that it’s not uncommon for neurological disorders to be misdiagnosed as psychiatric conditions. A few estimates suggest that about 15-25% of individuals initially diagnosed with schizophrenia may actually have an underlying neurological condition, though this figure can vary widely depending on the specifics of the study and the healthcare setting. In some cases, lesions or inflammation are only discovered after further neurological and pathophysiological testing (e.g., brain imaging, MEG, EEG and inflammatory marker evaluation), which can shift the diagnosis.
However, it’s worth noting that schizophrenia has a distinctive clinical picture, and misdiagnosis tends to occur more often in cases where symptoms are atypical or the neurological signs are subtle. When there is clear evidence of brain lesions, seizures, or other neurological symptoms, a more comprehensive diagnostic approach (including imaging) usually helps differentiate between psychiatric disorders and neurological conditions.
Cerebral inflammation can indeed cause symptoms that may be misdiagnosed for psychotic disorders, especially when the inflammation affects areas of the brain responsible for cognition, mood, or perception.
Conditions that cause inflammation in the brain—such as autoimmune disorders, infections (e.g., encephalitis), neurodegenerative diseases, endocrine disorders or even conditions like multiple sclerosis—can lead to psychiatric symptoms such as delusions, hallucinations, mood swings, and confusion. These symptoms can overlap with those seen in psychotic disorders like schizophrenia or bipolar disorder with psychotic features.
Misdiagnosis and how it can be avoided:
Overlap of Symptoms
Inflammation in the brain can cause hallucinations, delusions, agitation, and paranoia, which are core symptoms of psychotic disorders.
Disorders like autoimmune encephalitis can cause severe mood swings, depression, or mania, which can sometimes be mistaken for mood disorders with psychotic features.
Problems with memory, concentration, and thinking (often seen in inflammation-related brain conditions) can be confused with cognitive symptoms seen in psychotic disorders.
Differentiating Between the Two
To avoid a misdiagnosis, it’s crucial to conduct a comprehensive medical evaluation. This should include a detailed history (e.g., recent infections, autoimmune history, or neurological symptoms), a physical exam, and neuroimaging (like MRI, MEG, EEG or CT scans) to look for signs of brain inflammation or structural abnormalities.
Certain blood tests or cerebrospinal fluid (CSF) tests may help identify markers of inflammation or infection in the brain. Elevated levels of certain proteins or antibodies can be suggestive of neuroinflammatory conditions. In some cases, cognitive testing can help distinguish between psychosis due to a psychiatric disorder versus cognitive dysfunction related to brain inflammation.
Sometimes, clinicians will assess how the patient responds to treatments. If psychosis is related to inflammation, it may improve with steroids, immunotherapy, or antiviral medications, which are typically ineffective for primary psychiatric disorders.
Specific Conditions to Consider
One condition that commonly mimics psychiatric disorders is autoimmune encephalitis, which can cause rapid onset psychosis, mood disturbances, and confusion. Testing for autoantibodies (like anti-NMDA receptor antibodies) can help in diagnosing this condition.
Infections such as encephalitis, meningitis, or even HIV/AIDS-related encephalopathy can cause psychiatric symptoms and should be ruled out.
MS can sometimes cause psychiatric symptoms like depression, anxiety, and psychosis due to demyelination in certain brain areas. This can be distinguished from primary psychotic disorders through MRI scans showing characteristic lesions.
Minimizing Misdiagnosis
A team approach involving both neurologists and psychiatrists can help ensure a more accurate diagnosis when symptoms overlap.
A careful review of a patient’s medical history, including autoimmune conditions, infections, or a history of trauma, can help guide clinicians toward the right diagnosis.
If symptoms of psychosis arise suddenly or change in an unusual manner, it can raise suspicion for a medical cause rather than a primary psychiatric disorder. The timeline of symptom onset, course, and any precipitating factors (like infections or medications) should be taken into account.
Ultimately, a comprehensive diagnostic workup is essential to distinguish between cerebral inflammation and psychotic disorders. Early recognition and treatment of conditions causing brain inflammation can prevent further complications and ensure that patients receive the most appropriate care.
Link to Endocrine Disorders:
If a cavernoma is located near or within areas of the brain involved in endocrine regulation, it could theoretically contribute to endocrine dysfunction. These areas include:
Hypothalamus: The hypothalamus plays a central role in regulating the endocrine system via its control over the pituitary gland. A cavernoma in this region could disrupt hormone regulation and lead to a variety of endocrine disorders, such as:
Hypothalamic dysfunction (e.g., issues with temperature regulation, hunger, or thirst).
Dysregulation of pituitary hormone release (e.g., corticotropin, growth hormone, gonadotropins).
Pituitary Gland: Cavernomas affecting or compressing the pituitary gland could lead to:
Hypopituitarism (reduced secretion of pituitary hormones).
Hyperprolactinemia (if pressure disrupts the inhibition of prolactin secretion).
Other imbalances depending on the specific hormones affected.
Other Brain Regions with Secondary Effects:
Cavernomas causing significant intracranial pressure, hemorrhage, or secondary damage might indirectly affect endocrine function by impairing brain structures or pathways.
Rare but Documented Cases:
Although cavernomas are not commonly associated with endocrine disorders, there are reported cases of cavernomas near the hypothalamic-pituitary axis causing endocrine dysfunction. These cases emphasize the importance of the cavernoma’s size, location, and potential for bleeding or compression.
Symptoms to Monitor:
If an individual with a cavernoma develops symptoms suggestive of endocrine dysfunction, such as fatigue, unexplained weight changes, menstrual irregularities, or growth abnormalities, a detailed evaluation is warranted. This may include:
Hormonal blood tests.
High resolution imaging studies like MRI to assess the cavernoma’s location and size.
Conclusion:
While cavernomas do not inherently cause endocrine disorders, those located in or near endocrine-regulating brain regions (like the hypothalamus or pituitary gland) have the potential to disrupt hormonal function. It’s essential to work with a neurologist and endocrinologist to address these concerns.
Elizabeth has a recognised endocrine disorder which can lead to the effects below. The two hormones (neurosteroids) allopregnanolone and pregnenolone may be affected by the disrupted endocrine function and the levels of these should be tested. I consider it unlikely they have even considered this just like they have ignored the inflammatory markers that can cause limbic encephalitis.
They ignore all of these studies even when they are written by their own people like Dr Shahpesandy. Lots of people are detained on wards who would be able to be discharged if they were given hormonal supplements and anti-inflammatories. Even Shahpesandy acknowledges that.
Idiotic prescribing of anti-psychotics will in some cases make endocrine dysfunctions worse and benzos given as prnrapid tranquillisation can cause limbic inflammation.
Low levels of allopregnanolone and pregnenolone can contribute to psychiatric symptoms, including mood disturbances and, in some cases, psychotic symptoms. These neurosteroids play essential roles in stabilizing mood, reducing anxiety, and modulating stress responses, and they can be impacted by certain endocrine disorders. Here’s a closer look at how these neurosteroids interact with mental health and endocrine function:
Allopregnanolone and Pregnenolone in Mental Health
Allopregnanolone is a potent positive modulator of GABA-A receptors, which are central to calming neural activity and reducing anxiety. It helps create a sense of stability in brain signaling, counteracting overstimulation and stress. Low allopregnanolone levels have been associated with anxiety disorders, depression, and increased stress sensitivity.
Pregnenolone serves as a precursor to other neurosteroids, including allopregnanolone, and has its own neuroprotective effects, including modulating NMDA receptors and potentially balancing dopamine and GABA neurotransmission. It has been studied in relation to schizophrenia and other psychotic disorders, as low pregnenolone levels may contribute to cognitive impairment and psychosis.
Potential for Psychotic Symptoms
While low allopregnanolone and pregnenolone levels alone aren’t generally thought to cause psychosis directly, a deficiency in these neurosteroids can create vulnerability to psychotic symptoms, especially in those with predispositions or other stressors.
Neurosteroids like pregnenolone have been linked to dopamine modulation. Dopamine dysregulation is a hallmark of psychosis, particularly in conditions like schizophrenia. Reduced pregnenolone levels may therefore impact dopamine balance and contribute to hallucinations, delusions, and thought disorders.
Some research also suggests that allopregnanolone may have a stabilizing effect on mood and perception; reduced levels might leave individuals more susceptible to stress, which in extreme cases could precipitate psychotic-like symptoms in vulnerable individuals.
Low Neurosteroid Levels and Endocrine Disorders
Adrenal insufficiency (e.g., Addison’s disease) and other endocrine disorders affecting adrenal or gonadal hormones can reduce the availability of precursors needed for neurosteroid synthesis. This can lead to low levels of allopregnanolone and pregnenolone.
Disorders of the hypothalamic-pituitary-adrenal (HPA) axis, including chronic stress and HPA axis dysregulation, can also result in altered neurosteroid production. Chronic stress suppresses the production of pregnenolone and can shift steroid synthesis toward stress hormones like cortisol rather than neurosteroids.
Polycystic Ovary Syndrome (PCOS) and other hormonal imbalances involving estrogen progesterone may disrupt neurosteroid synthesis, as these hormones are involved in the pathways that produce pregnenolone and allopregnanolone. Individuals with PCOS, for example, have an increased risk of mood disorders, which may be partly related to altered neurosteroid levels.
Clinical Implications and Potential Treatments
Understanding low neurosteroid levels as part of a broader endocrine issue can help target treatments more effectively. Hormone replacement therapy (HRT) or neurosteroid analogs are sometimes used to restore balance in individuals with chronic deficiencies.
Pregnenolone supplementation has shown potential as an adjunctive treatment for schizophrenia and mood disorders, with some studies suggesting it can help reduce symptoms of anxiety, cognitive deficits, and even mild psychosis.
Similarly, allopregnanolone analogs, like brexanolone (approved for postpartum depression), are being explored for their potential to help with other mood and anxiety disorders, offering a novel approach to neurosteroid-based therapy.
Summary
In conclusion, low levels of allopregnanolone and pregnenolone can contribute to psychiatric symptoms, including psychosis, especially in individuals with underlying vulnerability. These deficiencies are indeed symptomatic of certain endocrine disorders, especially those affecting adrenal or sex hormones. Addressing neurosteroid imbalances through hormone therapy, neurosteroid analogs, or other supportive measures can be beneficial in managing symptoms linked to these deficits.
It is appalling that when you as a carer ask for pathological tests you are up against huge bullying and then safeguarding against you. There is no safeguarding towards the vulnerable person who needs the extensive pathological tests or for anyone whose diagnosis is in doubt denied such tests for many years. I know I am not alone in this matter and in the Scrutiny Meeting Minutes it actually highlights a national problem that needs urgent changes as if ignoring the necessity for such tests as so many lives are put at risk.
There has been a Community -‘style’ review organised, a second one, the first held last year excluding everyone in the family. This time I have written to Ms Amanda Pritchard of NHS England out of concern as it would appear nothing has been arranged fairly and I see this as a safeguarding concern.
What is a CTR?
I printed off the Care and Treatment Review Code and Toolkit (A Guide for commissioners, panel members and people who provide support). I then read carefully through each Standard and Principle. I would recommend every parent and carer print off this guide and check that the CTR is being arranged correctly and that they are included.
The purpose of a CTR Code and Toolkit is to provide a solid framework for CTRs in order for them to be delivered to a consistently high standard across England. Unfortunately, I am critical in respect of the way the CTRs have been arranged. I feel what is the point of them if they are not arranged properly and inclusive of the family/carers. The CTR is focussed on people who have been, or may be about to be admitted to a specialist mental health/learning disability hospital either under the NHS or independent sector and the ‘spirit’ in which they are carried out is paramount and rooted in principles of human rights, person-centeredness and co-production.
KLOE
Does person need to be in hospital?
Is person receiving right care
Is person involved in their care and treatment?
Are the person’s health needs known and met?
Is the use of any medicine appropriate and safe?
Is there a clear, safe and proportionate approach to the way risk is assessed or managed?
Are any autism needs known and met?
Is there active planning for the future?
Are family and carers being listed to and involved?
Are person’s rights and freedoms being protected and upheld?
It is the fourth year of detention and prior to moving she was living peacefully in the community compliant with treatment. I cannot see any of these questions, standards of principles being included in a CTR style review which I think is a complete and utter waste of time and none of the panel appear to be completely independent as I have checked.
It is supposed to be Person Centred but instead of this it would appear that institutional plans overall everything. There is no communication and with family excluded it gives me no hope that this CTR will result in fairness towards Elizabeth taking her wishes into account which is why I have turned to NHS England – Amanda Pritchard to scrutinise what is going on. Elizabeth’s wish is to come home to her independent bungalow next to family home.
The Standards are really interesting:
1.1 – Person and their family will be given information about the CTR in advance. Oh no they haven’t!
1.5 – Panel will make time available to meet separately with person and their family carer. Nothing properly arranged here.
3.1 – Where concern person’s human rights may not be being upheld. This is most certainly the case all along.
3.2 – Advocacy – provision of independent advocacy. There is no trustworthy independent advocate whatsoever as the advocates employed by the Trust have breached confidentiality in a capacity assessment on “Whether or not to have any Contact with Mother”.
3.3 – CTR will ask about legal framework for purpose eg at tribunal. THERE IS NO LEGAL REPRESENTATIVE EVEN THOUGH ELIZABETH HAS TRIED SEVERAL TIMES TO PHONE SOLICITORS – HER PHONE TAKEN AWAY AND HELD SECURELY, IN BREACH OF ART 8 HRA AND ALL CALLS SUPERVISED AND RECEPTION OF HER PHONE IS NOT GOOD. IT WOULD SEEM HER RIGHTS TO LEGAL PRIVILEGE ARE BEING OBSTRUCTED AS CALLS ARE SUPERVISED AND NO PRIVACY ACCORDING TO ELIZABETH.
4.1 CTR should take a day to complete. So in that case why have I just been invited for half an hr?
4.3 People supporting person should be at the CTR inc LA So could that be why I am only invited for just half an hour I wonder?
4.4 Physical health and general wellbeing. Private scans I paid for have indicated an anomaly (possible lesion) in the right hemisphere of the brain in an area where the meso-limbic pathway is located.
This lesion could be seen using the NHS approved DICOM (Digital Imaging and Communications in Medicine) an internationally recognized standard for storing, transmitting, and viewing medical imaging data, including MRI brain scans. The NHS and many healthcare systems worldwide rely on DICOM-compliant software to ensure interoperability between imaging devices and systems.
In Elizabeth’s scan the apparent lesion could be observed in three planes and triangulated to an exact position in the brain. The anomaly (lesion) appeared in the Axial Plane (Top to Bottom):
Also called the transverse plane, this section runs horizontally through the body, dividing it into superior (top) and inferior (bottom) sections.
The image was also visible in the Coronal Plane (Front to Back). This plane runs vertically, dividing the body into anterior (front) and posterior (back) sections.
And in the Sagittal Plane (Side to Side) This vertical plane divides the body into left and right sections.
A mid-sagittal plane runs exactly in the middle, splitting the body into equal left and right halves. A para-sagittal plane is offset from the midline.
The potential lesion is found at the right of the interhemispheric fissure in the sagittal plane, and of the superior in the axial plane and slightly to the anterior on the coronal plane
DICOM ensures that imaging data from MRI, CT, X-rays, and other modalities can be stored, transmitted, and viewed across various systems and software platforms.
It is widely adopted in healthcare, including within the NHS, for handling medical images.
The NHS uses a range of DICOM-compliant software and systems for viewing and analysing MRI scans. These include Picture Archiving and Communication Systems (PACS) and specialized imaging software.
Examples of DICOM-compliant software used in the NHS might include systems like GE Healthcare’s Centricity, Siemens Syngo.via, or Philips IntelliSpace Portal, among others. These are integrated with hospital IT infrastructure for seamless operation.
Under the circumstances it is necessary to re-examine this lesion under a higher resolution scanner such as the TESLA 3 or better still NEG TESLA 7 Phillips wide aperture scanner as this will improve acuity of image and reduce stress induced artifacts on the scan.
A brain lesion in the limbic pathway can potentially contribute to the development of psychotic symptoms. The limbic system, which includes structures such as the hippocampus, amygdala, thalamus, hypothalamus, and parts of the prefrontal cortex, plays a critical role in regulating emotions, memory, and behaviour. Damage or dysfunction in this system can disrupt these processes and lead to symptoms often associated with psychosis, such as hallucinations, delusions, or significant disturbances in thought and emotion.
There are a number of mechanisms linking limbic lesions and psychosis
Disrupted Emotional Regulation:
Damage to the amygdala or its connections can lead to abnormalities in emotional processing, potentially contributing to the paranoia or heightened emotional responses often seen in psychosis.
Impaired Memory and Cognitive Integration:
Lesions in the hippocampus or associated structures may interfere with the proper integration of memories and reality, possibly leading to delusional thinking.
Altered Dopaminergic Pathways:
The limbic system is closely connected with dopaminergic pathways, particularly the mesolimbic pathway. Lesions could dysregulate dopamine activity, which is strongly implicated in psychotic disorders like schizophrenia.
Disconnection Syndromes:
Lesions disrupting connectivity between the limbic system and prefrontal cortex could impair judgment and reality testing, leading to psychotic symptoms.
Neuroinflammation or Secondary Effects:
Lesions causing neuroinflammation or altering the surrounding brain environment can affect nearby circuits and neurotransmitter systems involved in psychosis.
Clinical Considerations:
Location of Lesion:The specific area and extent of the damage are critical in determining the likelihood and type of symptoms.
Co-occurring Factors:Pre-existing vulnerabilities, such as genetic predisposition, previous psychiatric history, or concurrent neurochemical imbalances, may increase the risk of psychosis.
Symptom Presentation: Depending on the nature of the lesion, psychotic symptoms might manifest in ways distinct from primary psychiatric disorders like schizophrenia.
While not every lesion in the limbic pathway will result in psychotic symptoms, there is a clear neurobiological basis for how damage to this area could contribute to psychosis. Such cases would require multidisciplinary management, combining neurology, psychiatry, and possibly neuropsychology, to address both the underlying neurological damage and the resulting psychiatric symptoms
So how on earth can a CTR ‘style’ review properly take into account all of this in a short space of time? I will ask this question to Ms Pritchard as it is most important to do these tests properly under the correct scanner.
5.10 CTR to question whether person’s care and treatment could be delivered in a non hospital setting.
YES – HOME! – How comes it is so difficult for this area to provide what was previously given in the former area. In that case then it would be cheaper to offer the private physical healthcare in the community and I as mother and carer could ensure attendance at all appointments which will save a lot of money. So much has been unnecessarily spent on wrong environments of care so far. Home is the right environment and there is so much scope for care to be provided in the home environment too unlike before.
6.3 Commissioner to write a report that all involved can understand and to ensure FAMILY AND CARERS AND OTHERS WHO NEED A COPY GET THIS WITHIN TWO WEEKS.
I am still waiting for the last report from last year and minutes. Where are these documents?
I have been invited at Elizabeth’s request to attend the CTR so I should be invited at 9.00 am until 5.00 pm not just for half an hour. This is ludicrous.
The last CTR was held in a secretive manner excluding all family and therefore nothing was done correctly and then according to Elizabeth two women approached her to tell her she was to stay where she was on the ward. No way was this done properly.
I particularly wish to be included in SECTION 7.
Section 7 gives guidance on exactly how things should be organised. The time allocated is still not enough time from between 10.30 am – 3.00 pm when the actual meeting started at 9.30 am. It says very clearly “meet with person AND THEIR FAMILY”.
A new advocate needs appointing because the current firm of advocates have breached confidentiality and I have had to complain quite rightly so. I am still waiting for my response in this respect.
According to the example the CTR ends at 5.30 pm. Especially important are the following points:
Am I safe
What is my current care like
Is there a plan for my future
Do I need to be in hosplital for my care and treatment.
The Expert by Experience is NOT independent.
There should be someone independent of the Trust as the the advocatelike there was in the former area where the CTR was done correctly.
There is no mention of the Neurologist or attendance by an Endocrinologist and this is extremely wrong.This means that a despite the Transforming Care Minutes no consideration is being given to physical healthcare.
To exclude a parent and carer is extremely wrong and there is no better Expert of Opinion than a parent and carer.
If parent and carer has serious concerns on physical health as well as health and safety on treatment and the way capacity assessments have undertaken as well as safeguarding and risk assessments, then these concerns should be taken on board and taken seriously instead of being ignored. This is why the CTR should be externally scrutinised as I see this as a safeguarding concern where person, their carers and parents are dismissed like rubbish when they have valid concerns and also when there are any doubts on physical health backed by scans going back to 2007. Nothing should be left to chance if there are seizures and other evident endocrine disorders. Every person should be allowed a second opinion under Martha’s Rule and just because they are held under the MHA is no excuse to ignore the urgency of such tests. The problem is that when you as a carer dare to question and ask for pathological tests then you get backlash and bullying.
In the former area Elizabeth was properly supported for the CTR and for the first time ever before we moved they were taking her physical health very seriously. All appointments were cancelled upon moving and instead, priority was to get rid of me as the NR and try and revoke the POA as they are trying to do right now. The CTR informer area was cancelled three times before it was finally arranged correctly but Elizabeth was fortunate to have the support of NAS and Access Charity who ensured there was no cheating with the CTR. Here in Lincolnshire she has no external trustworthy advocate and therefore nothing will be done fairly like last time – a waste of time and with family excluded and no legal representation I can see absolutely nothing good in this CTR ‘style’ Review. In my opinion it is a complete and utter waste of time and geared not towards the vulnerable person’s wishes but whatever Trust and Council have contrive. I do not like the way they have tried to take away her autonomy by so many capacity assessments done incorrectly. The CTR, if arranged properly, would have been a great opportunity to communicate and discuss and resolve concerns on both sides but I see this as an underhand exercise where decisions have already been made in advance and all I want to see as a mother and carer is for my daughter’s wishes to be heard and acted upon even if it is on a trial basis in terms of her coming home and that is her wish – TO COME HOME AND TO SEE HER CAT! and be close to her family. There are plenty of opportunities in the local community for her to do everything on offer under a hospital which is not a home!.
Section 9 is a tick box check list that the Chair should ensure is based on the principles and standards laid out in the CTR Policy which is clearly is not.
Section 10 is about Discharge steps and standards. It mentions “where people are assessed as lacking capacity” “Best Interest process”. That is what they have been doing all along with Lincolnshire County Council involved from the beginning and their BI assessors but today there was no doubt that Elizabeth had capacity and even when she was drugged to the hilt at a previous hospital her wishes are still the same and that is TO COME HOME.
I have not even had a carers assessment since coming to this area. In respect of the person concerned this CTR is to ensure “someone will look at my living arrangements and make sure I do not lose my housing or right to benefits while in hospital” That somebody is ME! as her Attorney “who I would like to live with? What I want from my life? She wants to come home but certain others are trying to make out I am a bad person, this is commonplace and experienced by many carers – they try to collectively say that the relationship is bad, put safeguarding in place again you and just gang up and ruin your life by trying to label you as a “perpetrator and abuser” which is why the safeguarding and risk assessments need proper external scrutinising and safeguarding works BOTH WAYS!
I remember the discharge from former area from Wales to Northampton to a care home where practically all money was taken leaving just £30 pw and no support on managing financially and I have proof that this care home run by social services, rated good allowed her to go without food at weekends. Absolutely appalling which is why I have tried to provide a home for life – an independent detached bungalow for her. None of the care institutions in the community have worked and the urban environment of London was not good so it is completely different here. Some residents in these care institutions can be loud and any noise is very triggering for Elizabeth so a bungalow in a peaceful location is what is needed and the location of home is extremely nice and suitable. I know she could settle down in this area and that there would be no problems.
TRANSFORMING CARE
I am looking at the minutes held in July 2024 of the ADULTS AND COMMUNITY WELLBEING SCRUTINY COMMITTEE and this meeting is attended by the commissioner of the CTR and same panel as the CTR. How interesting, it states:
“Many older adults MAY HAVE BEEN MISDIAGNOSED WITH MENTAL HEALTH ISSUES FOR DECADES. Data was being gathered on these individuals, especially those with learning disabilities who tend to be identified earlier.” This is a huge safeguarding issue yet I as Mother and carer who wishes for pathological tests done on abnormal findings on scans going back to 2007 am being bullied right now – that is how I see it. These minutes have identified huge nationwide safeguarding issues that NHS England need to address at each and every area. I have now identified further safeguarding issues on how CTRs are carried out incorrectly, not taking into account all the standards and principles and a CTR should be concerned with physical health and underlying conditions which are not catered for under the MHA. Properly arranged CTRs not CTR ‘style’ reviews are needed, with independent panels and properly arranged and organised like that in the former area was.
These minutes identify a serious national issue apart from this with long waiting lists for neurodevelopmental services. Waiting times for diagnosis were up to a year. Well in Elizabeth’s case it is coming up to 4 years under Lincolnshire and back to 2007 in former area who refused to look into matters properly so I as Attorney and Mother had to pay privately to confirm everything. When you advise the outcome of such private tests under the MH they are just ignored under the NHS.
“Diagnostic processes involved multiple professionals and efforts were being made to streamline this process to reduce waiting times. ” THIS IS NOT GOOD ENOUGH as lives are being put at risk.
NO autism respite provision. However Elizabeth is not being recognised as someone with autism. It is however recognised within these minutes that girls and women often masked their symptoms leading to late diagnosis.
Housing needed to be addressed. Well I have addressed that issue with a detached bungalow.All that would be needed is shared lives carers or young student professionals to knock on the door like I provided privately in a scheme in the community once. This community though is completely different to London and totally caring with lots going on and work opportunities etc.
This is so true: ONE MEASURE NOT ACHIEVING TARGET IS REGARDING CARERS SUPPORTED IN LAST 12 MONTHS. I can only go by how I have been treated and would regard this as bullying. To ban you from visiting for months on end, to take away the phone, to try to isolate and stop contact by way of capacity assessment backed by her so called advocates is very sad and that is because I am asking for pathological tests that are urgently needed but being ignored.
ADULTS AND COMMUNITY WELLBEING SCRUTINY COMMITTEE AGENDA WEDNESDAY, 4 SEPTEMBER 2024.
I have the previous minutes also but note nothing has really changed from the last minutes and now I am seeing the names of those involved and the attendees.
1 Apologies for Absence/Replacement Members 2 Declarations of Members’ Interests 3 Minutes of the meeting held on 24 July 2024 5 – 8 4 Announcements/Updates 5 Lincolnshire Safeguarding Adults Board Update (To receive a report from Justin Hackney, Assistant Director – Adult Care and Community Wellbeing, and Richard Proctor, Independent Chair LSAB, which provides the Committee with an update on the current position of key areas of work being undertaken within the Lincolnshire Safeguarding Adults Board (LSAB)) 9 – 14 6 Service Level Performance against the Corporate Performance Framework 2024-25 Quarter 1 (To recive a report from Caroline Jackson, Head of Corporate Performance, which summarises the Adult Care and Community Wellbeing Service Level Performance against the Success Framework 2024-25 for Quarter 1) 15 – 38 7 Adults and Community Wellbeing Scrutiny Committee Work Programme (To receive a report by Simon Evans, Health Scrutiny Officer, which invites the Committee to consider its work programme) 39 – 46
Democratic Services Officer Contact Details Name: Tom Crofts Direct Dial 01522 552334 E Mail Address thomas.crofts@lincolnshire.gov.uk
Please note: for more information about any of the following please contact the Democratic Services Officer responsible for servicing this meeting • Business of the meeting • Any special arrangements Contact details set out above. Please note: This meeting will be broadcast live on the internet and access can be sought by accessing Agenda for Adults and Community Wellbeing Scrutiny Committee on Wednesday, 4th September, 2024, 10.00 am (moderngov.co.uk) All papers for council meetings are available on: https://www.lincolnshire.gov.uk/council-business/search-committee-records
12 ALL AGE AUTISM STRATEGY Consideration was given to a report and presentation introduced by Justin Hackney, Assistant Director – Adult Care and Community Wellbeing, and presented by Catherine Keay, Head of Commissioning for Mental Health, Learning Disabilities and Autism – NHS Lincolnshire Integrated Care Board, which provided the Committee with an overview of Lincolnshire’s All Age Autism Strategy. The Committee were fully guided through the predation at appendix A of the report. Consideration was given to the report and during the discussion the following points were recorded: Many older adults may have been misdiagnosed with mental health issues for decades. Data was being gathered on these individuals, especially those with learning disabilities, who tend to be identified earlier. The Integrated Care Board (ICB) funded services for 16-18 year olds, but there was a national issue with long waiting lists for neurodevelopmental services. Waiting times for diagnosis were up to a year, locally, and up to seven years elsewhere. Autism Champions were being rolled out across various sectors to promote reasonable adjustments. The goal was to have these champions in every sector, including shops and local authorities, to create autism-friendly environments. The Virtual Autism Hub, started in February 2024. It was involved in the children’s diagnostic pathways and provided grants to support groups, especially in underserved areas. Diagnostic processes involved multiple professionals, and efforts were being made to streamline this process to reduce waiting times. Many autistic individuals were academically high achievers but struggled with stress and anxiety. The Autism Hub aimed to provide support across Lincolnshire to help these individuals develop everyday functional living skills. There was no specialised autism respite provision. Most autistic individuals needing social care support fell under mental health services. Creative solutions, like organising hotel stays with care support, were being explored. The Council was also working on gap analysis to identify needs for respite care and other services. Increased awareness of autism had led to more referrals overall. However, girls and women often masked their symptoms, leading to later diagnoses. Efforts were being made to raise awareness about different presentations of autism. Housing for autistic individuals, especially those without learning disabilities, needed to be addressed. Ground floor accommodations were often required due to safety concerns. The joint accommodation strategy group was working on specific needs and bespoke tender processes for care providers. Page 6 3 ADULTS AND COMMUNITY WELLBEING SCRUTINY COMMITTEE 24 JULY 2024 Efforts were being made to improve data collection and understanding of prevalence and future demand. There was a significant number of unemployed autistic adults. Efforts were being made to support these individuals into employment, but there was also a need to educate employers about hiring autistic individuals. There were disparities in the availability of support across different areas, with more resources concentrated in Lincoln. Efforts were being made to address these disparities and provide more equitable support. RESOLVED
That the report and presentation be noted, and the Committee’s support for the Lincolnshire All-Age Autism strategy 2023-28 be recorded.
That an update on actions and improvements be reported to the Committee next year. 13 SERVICE LEVEL PERFORMANCE AGAINST THE CORPORATE PERFORMANCE FRAMEWORK 2023-24 QUARTER 4 Consideration was given to a report by Caroline Jackson, Head of Corporate Performance, which invited the Committee to consider the Service Level Performance against the Corporate Performance Framework 2023-24 Quarter 4. It was reported that 95% of measures were achieving or exceeding targets. One measure that was not achieving target – regarding carers supported in the last 12 months. It was recognised that this target was giving flawed indication and was scheduled needed to be reviewed in the 2024-25 framework. Consideration was given to the report and during the discussion the following points were recorded: The Committee recognised that Lincolnshire was performing well when compared to statistical neighbours; however, improvements and progress should nonetheless continue to be made. Assurances from the Care Quality Commission were welcomed. It was understood that new standardised formatting for presenting data needed to be implemented so as to ensure effective benchmarking with other authorities. Client-level data was growing as a resource, which presented opportunities to inform and improve service delivery via a more sophisticated interrogation of data. The 2024-25 framework remained largely unchanged from the previous version. The following changes had been made: o PI31 – definitions had been revised. o PI111 – the target had been increased due to the expected expansion of the service. o PI59 – the target had been reset to give a better reflection of the service and meaningful intent. o Three additional contextual measures had been added: Page 7 4 ADULTS AND COMMUNITY WELLBEING SCRUTINY COMMITTEE 24 JULY 2024 PI194 – Personal wellbeing estimates – life satisfaction; happy; worthwhile. PI195 – Annual concentration of air pollution, fine particulate matter. PI196 – Percentage of households in an area that experience fuel poverty. Contextual measures were measured by questionnaires and survey but concerned subjective matters. Trends and trajectories could be garnered from these measurements to inform the direction of the service. Matters such as measuring air quality had an overlap between the two tiers of local government in Lincolnshire. RESOLVED
That the report be noted, and the Committee’s satisfaction be recorded.
That the 2024-25 Adult Care and Community Wellbeing Service Level Performance Indicators and Targets be supported. 14 ADULTS AND COMMUNITY WELLBEING SCRUTINY COMMITTEE – WORK PROGRAMME Consideration was given to a report by Simon Evans, Health Scrutiny Officer, which invited the Committee to consider its planned work programme. No changes had been made since publication; however, it was suggested that the following two items be moved from the September meeting on to October: Day Services Update Director of Public Health Annual Report 2023: Follow Up RESOLVED
That the report be noted.
That the above changes be made to the work programme. The meeting closed at 11.30 am Page
Elizabeth has asked many times to work in the hospital cafe but still she has not been given the opportunity. In this area there are many opportunities with the local college and hub for autism although Elizabeth’s condition has not been identified as Autism and she is being treated as a MH patient. She is now being taken out on group leave which she enjoys however I would compare the Trust to like a religious cult who restrict and deny family contact to any parent who dares to challenge and it is not the right thing to do when that family member might have extremely valid concerns.
I do not see any members of the public invited to this scrutiny meeting but I remember once when I turned up at the former area’s scrutiny wellbeing meeting I was told it was not open to the public. I had even offered to do the minutes. Doing the minutes accurately is what is needed which is why I should be invited ALL DAY to the CTR. I wonder what the response will be if I turned up to this Council’s Scrutiny Meeting.
Now having read these minutes I think the best thing is to do the entire safeguarding openly and transparently especially as regards why I am supervised 2-1 after all this time which is putting a huge risk on the ward and their staffing levels. Safeguarding works both ways and should not just be done on a parent and carer in such an underhand manner.
The CTR is arranged for the 30th of January and I have written to NHS England about this and also asked for my invitation to be all day and for the whole thing to be rearranged properly with a completely independent panel.
The Commissioner/Chair along with another Safeguarding Professional based under the Primary Care Trust are giving the most interesting talks to Lawyers on “Challenging Families and Best Interests” How to manage challenging families!”
In answer to that – there would be no such a thing as a challenging parent and carer as if they were listened to, included and treated with respect then this would enable Trusts to work effectively in determining what is in the best interests because after all, a parent/carer is the only EXPERT BY EXPERIENCE.
I will never forget the comments of the Independent Chair of the CTR done correctly under former area. He said “The whole thing stinks!” How true! However the former area were going to send Elizabeth to the Priory in Hemel Hempstead but instead her wishes were listened to and she was allowed home. Unfortunately it is like going backwards in this area as there is no communication and families/carers are treated as though they are invisible – if this is how I am being treated there must be others. The minutes of these scrutiny meetings look like they contain same matters which have just been copied and pasted but these people are not properly safeguarding my daughter who urgently needs pathological tests after so many years of neglect from former area and current where we had hoped so much for a fresh start. Instead, it has been one hell of a nightmare and still ongoing after so very long but now disturbingly with all the attempts to revoke the POA yet again there is much going on behind everyone’s backs right now and no answer from the Public Guardian Office as yet. I will keep you all informed and these meeting should include parents and carers after all it is a scrutiny meeting.
Today i have spent quite some time trying to get through to Sheffield Hallamshire Hospital where my daughter who is held a virtual prisoner under Castle Ward can have the extensive tests she needs on her physical health which the MH would appear to be obstructing. Elizabeth is having seizures that are frequent. Her Responsible Clinician says I am partly to blame for such seizures and there are heavy restrictions in place on just me right now visiting my daughter with 2-1 supervision and not allowed any time with my daughter to take her even in the hospital grounds. This is bullying to the extreme by Lincolnshire Partnership Trust. It is also huge neglect as all they have done is cancel referrals already made by a previous area that the new GP said I should take her to. Everything was put in the way of that at Ash Villa, the previous hospital. Now the RC has put massive restrictions in place contrary to the health and wellbeing of my daughter.
Elizabeth is going downhill. Her face was a mass of red blotches and forehead looked as though she had hit her head on the wall or door – a hard surface. Her knuckles were encrusted with scars that had obviously healed from bleeding. She said she had been injected again recently. She started having the seizures at Ash Villa and there was a cancer scare – they say tests for came out normal. I had private scans done. I sent them to various experts on disk and all said the same thing that certain images need to be closely investigated by Neurology. You can imagine how happy I was when finally she was referred to a Neurologist under United Lincolnshire Partnership Trust. On the 3 January was supposed to be her appointment. She was not taken there by the MH team. I turned up instead with the private scans I had done in a small window of opportunity because for the most part LPFT have stood in the way of all leave and visits highly restricted. It is almost as if they are trying to protect themselves or know more than they let on. There is clearly something physical wrong for my daughter to have such frequent fits. She is not being monitored for her blood oxygen levels and following each fit they give lorazepam which is extremely wrong so I have been told. If she has temporol lobe epilepsy the treatment would be different but Elizabeth is treated as though she is a MH patient and nothing else. LPFT have ignored all the screenings and all the past assessments done by Huntercombe who claimed she had high functioning Aspergers. That was back in 2017 under Enfield. It would appear that ALL the doctors seem to be protecting each other because today I have had to go to enormous lengths to write and enquire about these scans. Because of my grave concerns about my daughter’s wellbeing and safety on the MH ward (Castle Ward) Lincolnshire – no way should it be left to a team of MH professionals to film my daughter against her wishes having seizures. This is against GMC guidelines. Secondly her capacity is highly disputed. There are three flawed capacity assessments done purely for the purpose of getting rid of me as nearest relative which they succeeded in. All are heavily flawed and not in line with Principle 4 and Masterman-Lister case and they do not take into account the causative nexus. The causative nexus is highly important to see determine impairment. This has not been done, making all three capacity assessments not fit for purpose.
I finally got through to Sheffield who told me that absolutely nothing had been arranged. The person concerned when to some lengths to check and refer to a supervisor.
It is hard to trust anything the NHS does as when things go wrong there is nothing but a wall of silence and it is very hard to age any kind of justice even when someone dies as a result of negligence. There appears to be a wall of silence right now. Certain doctors (even those assigned to look at physical health) appear to be standing in the way of my daughter’s much needed physical health referrals which has been the case since we moved to this dreadful area of Lincolnshire. The word normal most certainly does not mean normal and they are depriving my daughter of the necessary physical health referral to a Neurological ward where she could have extensive tests done to determine the real reason for the fits and not rely on just observations and comments that state “it is the mother’s fault”. The reasons for my appalling treatment is because of “concerns” by her Responsible Clinician on my part and an entire MDT all acting ultra vires against their own code of conduct and treating Elizabeth as someone who has no capacity. LPFT HAVE COMPLETELY ABUSED THE MCA AND NOT GONE ACCORDING TO NATIONAL GUIDELINES. I am now a BI assessor myself and am frankly disgusted at such enormous dishonesty and in addition after all this time she has not had proper pathological tests or any psychological input. The law is failing to protect vulnerable people such as my daughter.
I have written to Pals today, the Neurological department of ULHT, care concerns (LPFT) and my MP and here are my emails below. You should not have to go to these lengths. Elizabeth agreed to go to Sheffield. There seemed to be more concern about her breaking expensive headgear which she promised not to break than her physical health and wellbeing and the necessity to have these extensive tests. This is highly negligent on the part of the NHS. ABSOLUTELY NOTHING ARRANGED FOR THE SECOND TIME as today I checked with Sheffield.
FOR THE ATTENTION OF DR S I would like an appointment to discuss my daughter’s care with you. I have today checked with Sheffield Hallamshire Hospital only to find out that NOTHING has been arranged. E is having life-threatening seizures and I visited her yesterday. I have grave concerns for her wellbeing. My daughter no longer wants to live. She was covered in red marks, she is having constant fits which ARE NOT mental health conditions. You are responsible for referring her to have extensive tests which Lynsey has agreed to have done. Why has this not been done? This matter is subject to a high court case right now. I would like to know your reasons for not referring my daughter to Sheffield or has she been referred elsewhere? I would like your reasons why a MH team should film my daughter against her wishes and that you should wish to take their word when they are not qualified to comment. I was assured by your department when I called last Wednesday that an appointment had been made and it has not as I have checked today. How can you possibly monitor my daughter when you are not there 24/7. I was also told by Sheffield to contact the GP which I have done. I would like to know the details of what exactly has been arranged.
Since moving all E’s Neurology appointments have been cancelled which is highly neglectful. She has had several accidents and her face was absolutely covered with red marks. I want my daughter to have the physical health checks she needs and under Martha’s Rule she is entitled to have this. Nothing has been arranged so I need to know all the details of the appointment to pass onto the court. Her condition in past files points to neurological not mental health. I look forward to hearing this information from yourselves and the GP. I have not had response to my emails from your department and I need that response today. Thank you. I am beginning to feel like no-one wishes for my daughter to have extensive tests done and are ignoring her physical health completely. It is also against GMC guidelines to film a patient who has said she does not wish to be filmed. Not having these tests done is preventing my daughter for being evaluated on her capacity ie the causative nexus which is subject to high court action right now. Yours sincerely
Susan A Bevis T
From: susan bevis Sent: 22 April 2024 11:19 To: PALS (ULHT) pals@ULH.nhs.uk Cc: NEUROLOGYSECRETARIESLINCOLN (UNITED LINCOLNSHIRE HOSPITALS NHS TRUST) ulh.tr-neurologysecs.lincoln@nhs.net; MARISCORECEPTION (NHS LINCOLNSHIRE EAST CCG) LECCG.MariscoReception@nhs.net; Subject: Elizabeth Bevis For the Attention of Dr S (Case Ref: VA18567)
TO WHOM IT MAY CONCERN
I need to know the full details of the referral that was meant to be done on two occasions now to Sheffield for E to have an MRI scan done under a Tesla 3 scanner. On two occasions now I have phoned sheffield because no-one is responding to my emails. No appointment has been made on two occasions now despite assurances. I therefore need a copy of the referral details as obviously I cannot go by their word. I have spent a long time trying to get through only to be assured that absolutely nothing had been arranged.
Please therefore let me know the details of the referral and if this referral has gone to another area such as Nottingham by any chance?
I look forward to hearing from you regarding this urgent matter.
When I came to Dr S clinic last Wednesday I did not have an appointment arranged and did not expect to barge in front of others. I explained that no appointment had been made for Sheffield. Two ladies (managers) came out to see me witnessed by ******* All they could do was pass messages on to Dr S. I was then assured that the necessary appointment for E to go under a Tesla 3 scanner had been made. i had explained that nothing had been arranged previously and that this was being looked into and that a referral had been made when it had not been made according to Sheffield. I am absolutely in despair to hear yet again Sheffield have no record of any appointment or referral even being made.
Please can you look into this matter and provide me with details of the appointment. It is almost as if noone wishes my daughter to go and have the extensive tests needed and are trying to play down the necessity of it all.
The seizures are life threatening, the MH team are not monitoring her blood oxygen levels properly. She is being treated in the most appalling manner. I am scared for my daughter’s life. The referral to Sheffield was meant to extensively look into my daughter’s physical health and wellbeing and yet again for the second time nothing has been arranged. I totally despair.
I need to know the full details of the appointment as under Martha’s Rule my daughter is entitled to a second opinion and this can only be achieved through extensive tests done through Sheffield.
This is now urgent. I need full details of the appointment they claim had been arranged yet no-one is responding to my emails under the Neurological department of Dr S.
Yours sincerely
Susan A Bevis
2.5 years of appalling imprisonment under the barbaric NHS where not one person takes responsibility.
Everyone working together to cover their backs in the form of MDT that goes way beyond nursing and doctors codes of conduct.
Total conflict of interest at Board level with no-one taking responsibility.
In the middle of this mess is a vulnerable person now covered in marks, scratches where she is obviously totally distressed and injected frequently, missing meals and that in itself is dangerous and to make up for missing meals is taken to the shop where she may buy crisps and snacks to compensate. At least at home she would be looked after nicely and now she no longer wishes to live so she has told myself and others who have visited her.
She is treated as though she has no capacity and is being denied her physical health assessments which have not been referred as advised on two occasions.
Absolutely dreadful situation. No accountability and these doctors try to play down their responsibilities and try to put all the blame on you as a parent/carer instead of take an interest and investigate what could possibly be the cause of these life threatening seizures. To think they are more worried about her breaking equipment she is supposed to wear on her head to monitor properly than the wellbeing of my daughter.
Then I get an email from a Ms Lowe of Marisco Medical who has said she has been told not to answer my emails because I am writing to her via her own personal email address that states NHS/ICB but I just wrote back and said that can simply copy in by cc to her personal NHS email address the correct email address as what had been given to me had emails bounce back. I do not expect to hear anything but it is good communication to point out that this is the wrong email address and copy in the correct email address surely? She is supposed to be a lead safeguarding person under the GP surgery. This is a safeguarding matter they need to be aware of as two referrals have not been done. At least instead of dismissing such concerns the person should write more clearly and then why use a personal email address in the first instance to correspond with me then now say this is wrong?
So now I have to wait several days if not weeks before I get any kind of response I have asked for ie date of referral and details of what has been arranged. Why is that so difficult when Elizabeth has given consent and it seems like NOONE wants me to know anything.
In the meantime a Ms Emily Scott who is supposed to be the Clinical Lead for Castle Ward has told Elizabeth she is moving elsewhere or words to that effect that she is being taken to see a place but noone in the family is being advised of this and so the information is via Elizabeth.
When I visited Elizabeth she clearly said she wanted to come home, she misses her cat and misses her home and family. Elizabeth has spoken more than one of staff shortages on the ward and I have this in writing.
I am the only person who comes to visit each week without fail. My visits are heavily restricted 2-1. Even a prisoner is treated with more respect.
As regards capacity I had bought Elizabeth something where it indicated there was 9 pieces in a box. I had not eaten myself and after doing all her shopping for her had no chance because the visit was 2.30 and I had two pieces from that box myself. This shows tremendous capacity for Elizabeth to question where the other two pieces were. In addition to this I had bought all the nice things she wanted me to. Food is the only comfort for a patient treated like a caged animal you would see in a zoo. In a prison warders may be present and walk up and down but do not sit there taking notes of everything being said in a small cramped room, Ms Munro describes as “spacious”. So why are they doing this – it is on order. An Executive decision or that of the Responsible Clinician who is clearly not taking into account the fact that this is not conducive to recovery. It has not been taken into account that she would like some leave after all this time and only has 45 minutes so the only other enjoyment is going to the hospital shop and even that was used as punishment for appearing hostile, the subject at the time of an interlocutory injunction. This could not go forward due to county court not having the jurisdiction.
When a responsible clinician goes down the legal route first before medical concerns this is highly negligent. Why are they filming her on the ward having seizures and trying to make out this is caused by her mother. Why dont they do the responsible thing by refer her to sheffield and for the endocrinology tests as already proven in private tests there is dysfunction.
It would seem there are no standards and those at the top also work for the care quality commission and the ICB.
All I have ever wanted is for my daughter to be treated fairly.
Sadly I have chosen to live in a beautiful area that would benefit Elizabeth but she is not allowed any meaningful contact – there is complete abuse of human rights under this area. There is no accountability.
This is displayed by LPFT – what is a just culture exactly? This is completely ridiculous and biased. Just mention a “just culture” to all the parents and carers affected right now and particularly all the patients stuck on wards for years on end whilst Trusts such as this act dishonestly. When you dare to challenge you can expect a response as follows from the likes of Ms Munro who is as unfit to write complaint responses as the doctors who carried out the flawed capacity assessments.
Here is what Elizabeth has described her experience as: “hell on earth”. This is also how parents and carers view matters, those who are affected and those who are ignored. How can there be any accountability whilst those at the top have connections with the Care Qualilty Commission? How can any members of the public have faith in the Care Quality Commission who have produced some very dismissive responses even calling themselves a “business”. I have featured this on a former blog.
The Care Quality Commission (CQC) have asked us to respond to requests you have raised with them and clarify the Trust’s position on a number of points:
You have requested an apology for the verbal threats made by Dr Khokhar where she said “I am banning you indefinitely for inciting your daughter to attack members of staff on Xmas Day”.
Following the incident on Christmas Day 2023, the Trust followed the usual incident reporting and investigation processes, as well as complying with instructions and communication from the Police. During this period of investigation, your visits to the ward to see Elizabeth were suspended in line with the Mental Health Act Code of Practice 2015 and to ensure the effective delivery of Elizabeth’s care and treatment could be prioritised. Dr Khokhar accepts that he used the word “indefinitely” and that this could be seen as inflammatory. It was used to reflect that at the point, an end date to the restrictions could not be confirmed. However, the letter sent dated 29th December 2023 confirmed that the situation would be reviewed on 25th January 2024. After subsequent review of the relevant documentation, the visiting restrictions were lifted from the 5th February 2024.
You asked about your invoice for £50 for Elizabeth’s ‘wasted’ phone contract.
As previously explained in an email on 29th Februay 2024, Elizabeth’s phone access was limited for a fixed period of time as part of a comprehensive care plan that considered Elizabeth’s human rights. This was to ensure the response to her phone use did not adversely impact her engagement with, or the efficacy of, her treatment plan. This ceased on the 5th February 2024 following a review of all of the relevant factors. Elizabeth’s phone continues to be kept securely by ward staff and Elizabeth is able to request to use her phone at any time. In addition, ward staff regularly encourage Elizabeth to use her phone to maintain contact with family.
We monitor and document Elizabeth’s phone use to ensure that she has fair and reasonable access to her phone. This details the occasions when she has been supported to use her phone and make calls and evidences that Elizabeth continues to be able to use her phone on request . On the basis that Elizabeth does continue to use her phone, we would not provide any reimbursement for her phone contract.
You said that Elizabeth’s birthday cake was thrown away.
To ensure that the limited storage space for fresh food brought onto the ward by visitors is fairly available to all patients on the ward, a new process has been put in place. This is clearly communicated to patients and their friends and relatives when they visit to manage expectations. The ward also adheres to Trust wide infection prevention and control (IPC) policies relating to food storage and consumption to ensure patient safety. Elizabeth’s birthday cake did have to be disposed of on 15th February 2024 as the expiry date had been exceeded.
You raise concerns about the size of the visitor’s room and that it was cramped which upset Elizabeth
The family room on the ward is used for visits as it affords privacy and has CCTV available which can be used to review the area, if necessary. This room is the largest room on Castle Ward used for visitors.
Subject Access Requests
In relation to the Subject Access Requests (SARs) received both for personal data relating to yourself and requesting a copy of Elizabeth’s rapid tranquilisation healthcare records, the Trust’s position remains the same as detailed in the email sent on 11th December 2023. This is because we are of the view that your request is “manifestly unfounded or excessive” as detailed in Article 12 (5) of the GDPR.
Our Records Management team did note that you subsequently attached a consent form from Elizabeth. However, this was not the correct consent form to support your Subject Access Request. Further, we continue to have concerns regarding Elizabeth’s capacity to consent, which has historically remained interchangeable with regards to information sharing. We also have continued concerns that any information shared may, in turn end up within a public forum which is outside the scope of any consent that we may gain.
We ;have provided a copy of this letter to the CQC.
Yours sincerely
Ann Munro
Patient Experience Lead
Cc Care Quality Commission (Central) Citygate, Gallowgate, Newcastle Upon Tyne
NE1 4PA
EXTRACTS FROM MY RESPONSE EMAIL TO MS MUNRO’S LETTER.
Yr Ref MHA-011217-X6F7T0
Dear Ms Munro
CEO (Sarah Connery) on the Trust’s Executive Board also works/worked as a Specialist Advisor for CQC or The Director of Operations (Chris Higgins) who works/has worked as an Executive Reviewer for CQC
Thank you for your letter of 4 April.
When you mention “The Care Quality Commission” asked you to respond. Who might that be? Could that be either of two LPFT Board Executives mentioned above by any chance? To think, all this time so it would appear LPFT have been answering on behalf of the Care Quality Commission in a defensive, almost threatening manner. What a conflict of interest! No wonder why none of my complaints have been dealt with satisfactorily and with Mr Higgins as Executive Reviewer for CQC it is also no wonder why you are rated “good”.
How can you have a CEO (Sarah Connery) on the Trust’s Executive Board who also works/worked as a Specialist Advisor for CQC or The Director of Operations (Chris Higgins) who works/has worked as an Executive Reviewer for CQC however I am talking about LINCOLNSHIRE PARTNERSHIP TRUST WHO APPEAR TO HAVE THEIR OWN LAW TO SUIT THEMSELVES.
I would like your opinion on this conflict of interest, Ms Munro.
Regarding your third paragraph I would point out this was the third time Police were called unnecessarily, all done for the purpose of threatening and intimidation however Section 9 statements were done to back the truthfulness of events on Xmas Day to cover our backs. What a waste of Police time. It is obvious that the restrictions are still ongoing with HCA’s/nurses writing notes during visits (no doubt of an adverse nature). This is bullying to the extreme to stop visits and threaten to do so indefinitely but still continue with restrictions. You might like to write a statement t explaining exactly what you mean by “suspension in line with the MHA Code of Practice”: Please also explain why I am being treated differently to everyone else which is discrimination.
Here is the MHA Code of Practice relevant points which were not even quoted in full as a reason to ban my visits.
MHA CODE OF PRACTICE
Restrictions or Exclusion on Clinical Grounds
11.14
From time to time, a patient’s Responsible Clinician may decide, after assessment and discussion with the MDT, that some visits could be detrimental to the safety or wellbeing of the patient, the visitor, other patients or staff on the ward.
In these circumstances, the Responsible Clinician may make special arrangements for the visit, impose reasonable conditions or, if necessary, exclude the visitor. In any of these cases, the reasons for the restriction should be recorded and explained to the patient and the visitor, both orally and in writing (subject to the normal considerations of patient confidentiality). Wherever possible 24 hour notice should be given of this decision.
Restriction Or Exclusion on Security Grounds
11.15
The behaviour of a particular visitor may be disruptive in the past, to the degree that exclusion from the hospital is necessary as a last resort. Examples of such behaviour include:
Incitement to abscond
Smuggling of illicit drugs or alcohol into the hospital or unit
Transfer of potential weapons
Unacceptable aggression
Attempts by members of the media to gain unauthorised access
11.16
A decision to exclude a visitor on the grounds of their behaviour should be fully documented and explained to the patient orally and in writing.
Where possible and appropriate the reason for the decision should be communicated to the person being excluded (subject to the normal considerations of patient confidentiality and any overriding security concerns.
LPFT ARE IN BREACH OF THE MHA CODE OF CONDUCT RE: THE FOLLOWING POINTS:
“may make special arrangements for the visit” : No special arrangements were ever made and contact severely restricted by taking the phone away that affected the entire family and was detrimental to Elizabeth – depriving her of her phone deprived her of contact with everyone else in the family and was done primarily to punish me and deprived Elizabeth of listening to her music. This is in breach of human rights and totally degrading and undignified to Elizabeth..
“the reasons for the restriction should be recorded and explained to the patient and the visitor, both orally and in writing”.: None of this was done properly explaining the grounds mentioned below for banning visitors. No Impact assessment carried out as should have been.
“subject to the normal considerations of patient confidentiality). Wherever possible 24 hour notice should be given of this decision” This was not done. The pre-arranged visit was cancelled on the spot whilst Elizabeth stood the other side of the door – absolutely degrading and totally cruelty to do this without any notice. Nursing staff acting ultra vires upon orders at Executive level and against their own code of conduct.
None of the above was done properly and also LPFT failed to carry out an Impact Assessment which LPFT is supposed to do under NHS Guidelines and this should have been done on myself, on Elizabeth and a copy sent to the Nearest Relative. LPFT are therefore in breach of NHS Guidelines. Here below in bold are the justified reasons to completely ban visitors according to MHA Code of Conduct.
Incitement to abscond
smuggling of illicit dugs or alcohol into the hospital or unit
Transfer of potential weapons
Unacceptable aggression
Attempts by members of the media to gain unauthorised access
None of the above apply in my case.
Dr K cannot very well deny threatening me with an indefinite ban as this was witnessed. Having such a ban has had a detrimental affect on my health. Elizabeth’s face is covered in marks where she is distressed and has been self harming and has said on more than one occasion she no longer wishes to live which in turn affects my health. The missing of meals has continued beyond the last safeguarding and had happened constantly at Ash Villa in the past yet nothing was done. It is bullying to the extreme to ban visitors and that is the tactic that LPFT adopted. My visits were suspended on none of the grounds above. Elizabeth’s care and treatment has been atrocious. She has been missing meals, isolating in her room because she cannot stand the noise. She has been deprived of proper pathological tests and nothing has been arranged as regards Sheffield as I have checked. There is no way a MH team can do proper pathological observations and have been filming my daughter when she is having fits against her wishes. This is an absolute disgrace. The way the MCA has been abused is another disgrace on the part of LPFT who enlisted the assistance of the council in this respect at County Court that lasted months and months on end. Human rights are non existent under LPFT and have never taken into account of. My daughter’s human rights are being dreadfully abused. It is not true when you state visiting restrictions were lifted from 5 February 2024. Restrictions are very much ongoing and visits are not of quality time but intrusive and degrading due to constant supervision. I am being discriminated against because other family members do not have 2-1 restrictive visiting with members of staff writing notes. The restrictions still very much in place clearly have a detrimental affect on my daughter who is treated like a prisoner. She reacted on Xmas Day to staff taking notes constantly. Even on Xmas Day, human rights were ignored by LPFT. How would any of you like this kind of treatment? It is breach of Art 8, Art 5 and Art 3 HRA. Police time was wasted on Xmas Day and Elizabeth was thrown into seclusion and rapidly tranquilised when she became upset by a crowd of “professionals” waiting outside the visitor’s room who grabbed hold of her because she had shouted at the lady writing notes because it was totally distressing to her.
There have been two accidents apparently according to Elizabeth, one at Ash Villa and another on Castle Ward where she lost balance or hit her head badly. Why wasn’t anyone in the family notified?
Because we pay a phone bill each month and Elizabeth hardly gets any use of the phone it is only fair that LPFT compensates for this. The bill now stands at £60 for your information and I request settlement of this amount to Elizabeth as already advised. Every month she is restricted with her phone I am adding on to that bill. Also under Ash Villa the phone was taken away for weeks on end making it difficult for the entire family to get through and for Elizabeth to be able to speak to family members. The reason for this was because Elizabeth kept calling the Police in distress. It says so in file papers.
“Elizabeth’s phone continues to be kept securely by ward staff and Elizabeth is able to request use of her phone at any time.” That is in breach of human rights. Totally degrading treatment – shame on you LPFT! Is this care? or rather is it abuse of a vulnerable person and their rights – it should be the least restrictive care under the MH LPFT are abusing patient’s rights and if this is just my daughter then this would also come under the Equality Act 2010. No other patient is being treated in such a degrading manner as my daughter. It is not the point that she is encouraged to use her phone. She is not at risk from anyone in her family and therefore the restrictions are excessive and the kind of thing that would apply to a restricted prisoner not a patient under the MHA.
LPFT haven’t got a clue when it comes to human rights and this is why I am copying in the British Institute of Human Rights. To keep the phone locked away constantly is a disgrace and still ongoing to date. Elizabeth does not like the phone being monitored and she expressly said she did not want to be filmed so why has this just gone ahead?
You clearly do not know the meaning of “fair and reasonable” . Elizabeth is a grown adult of 37 years of age and does not need support to use her phone.
The Birthday cake was not given to Elizabeth on her Birthday and should have been given to her immediately as I specially came back to the ward. It was her Birthday and no respect was given to this special occasion. Elizabeth did not even know I had brought her the Birthday cake so once again there was no communication. At Ash Villa all her presents were just dumped in a storage room. She did not know they existed. I brought another cake to make up for this and again Elizabeth was not given it. The second time it was not fresh cream and I assume thrown away.
Yes, the visitors room is cramped when 2 people are listening to every word and crammed into the room. It is undignified and unpleasant to say the least. How can you possibly say the visitor’s room affords privacy in the circumstances. You just have no insight into the situation. The rooms are all small in nature – not much difference in size but because of the restricted visiting and note taking going on (no doubt adversely against me), it is an unpleasant degrading experience that even a prisoner does not have to endure. In a prison, warders walk up and down but give respect to prisoners at visiting times to have privacy to see their families. The ward is worse than prison and the treatment is degrading, abusive and aimed no doubt as punishment towards me, but inflicting upon my vulnerable daughter.
Subject Access Requests.
I know LPFT do not want me to see any records especially not the copy of the CP11 rapid tranquilisation log. All the files and notes being taken will be requested through ICO. You have no right to refuse such request from both of us.
Your capacity assessments are totally flawed. I want full safeguarding done externally because in the past safeguarding under LPFT resulted in “I am satisfied” response. The safeguarding should be especially looking into the flawed capacity assessments. I am now a BI assessor – everything LPFT has done is wrong. Your capacity assessments are not fit for purpose. LPFT have abused the MCA. It is most certainly of public interest that everything is addressed openly and transparently.
Finally, please ensure that my daughter gets all the pathological tests she needs under Sheffield as soon as possible as this is another area of safeguarding that needs to be thoroughly looked into. I believe safeguarding should be done on the deprival of medical referrals to my daughter for her physical health and referrals need to be made to spend a full week under Sheffield for everything she needs, including Endocrinology
I have to say, I have never encountered such bullying in all my life and such dishonesty. You have been rating yourselves as good yet there are tremendous conflicts of interest I have witnessed at Executive level.
The capacity assessments are useless without referral to Sheffield and according to Professor Keith Brown everyone should be included (including myself) with the capacity assessments undertaken. My daughter most certainly has capacity and she is being abused and no-one cares otherwise this situation would not have been left to continue for so very long.
Here are the guidelines to filming patients against their wishes:
Keith Brown. Editor. Demystifying Mental Capacity: A guide for health and social care professionals (Post-Qualifying Social Work Practice Series). First …
Mental Capacity Act 2005 :
(Section 4): Requires that patient to be regarded as having capacity until evidence ascertained as to how that capacity is impaired.
(Section 4) (1) (a) and (b): “The Prohibited Step” Decision maker should not draw conclusion on capacity from patient’s age, appearance or on a condition of his/hers or an aspect of behaviour which might lead others to make unjustified assumptions on what might be in his/her best interests.
(Section 4) (2): Decision maker should try to identify all issues most relevant to the individual relating to particular decision (para 3, Main Code of Practice).
(Section D): inconsistencies of witness statements on capacity. Capacity assessments not conducted as required by S1 MCA 2005
Masterman-Lister v Brutton & Co [2003] 1WLR 151
“a party to legal proceedings is capable of understanding, with the assistance of such proper explanation (in broad terms and simple language) from legal advisers and other experts as the case may require, the matters on which their consent or decision was likely to be necessary in the course of those proceedings.”
Dont bother providing a copy to the CQC as LPFT are the CQC defending yourselves and rating yourselves as good when in actual fact you should be rated as “Requires improvement” or “inadequate” and you can’t even offer an apology for the shocking abuse of my daughter and her family in terms of human rights which you clearly have no insight of.
My final question to you is have LPFT applied for DoLs and in the meantime waiting to hear from the court because your intention is to dump her into a care home out of area in say Yorkshire and restrict contact forever? Why is she still held without leave under the MHA for over 2.5 years deprived of family contact and proper physical healthcare? I would like to hear from any of you in this respect as this is absolute abuse and breach of the law and the question needs to be asked about the validity of the entire section that is ongoing and the dishonesty in arriving at such decisions to hold her a prisoner indefinitely. My daughter is one of thousands trapped under the MHA by appalling Trusts such as LPFT and dishonesty too on the part of Councils who do not wish to provide any support whatsoever in the community. In fact I was not asking for anything of this area which brings me to the question of residency status and whether that responsibility still remains the responsibility of Enfield?
I have already revealed Elizabeth’s scans which were done in November at Lincoln County Hospital with the result of “normal”. I would urge all of my readers to double check what scanner has been used as a 1.5 scanner has not picked up what is clearly visible on the private scans I had done through S G Radiology. I am waiting for an explanation as to what the images portray as I cannot accept these images to be normal. They even state “trauma” so as a parent or carer it is evident that you cannot always assume that normal means normal. A while back Elizabeth had an ultrasound as there were fears of cancer. Now I want all the scans done again under a Tesla 3. I have heard a Tesla 7 is even better and will look into where this can be done in the UK. So Lincolnshire, Enfield, Weston are just three examples where they do not have the up to date scanner and therefore you cannot rely on the results. This affects not just people under MH but everyone.
For so long now I have been trying to get answers – it clearly states “Anterior Region Medial Temperol Compromise which is not a mental illness and yet Elizabeth has been treated under MH with massive dosage of antipsychotics that do not work and is “treatment resistant” – poor/non metaboliser which I have prove by P450 tests. Now everything is falling into place and it is something I want to share with all of you especially those going through cancer treatment. Never trust the word “normal” and check what scanner your Trust has. I am currently asking my MP, Victoria Atkins why Lincolnshire does not have a scanner that is reliable. This means all of Elizabeth’s treatment may be affected as last year there was a cancer scare. Now I want all the scans/ultrasounds done through Sheffield and for Elizabeth to be referred to a Neurological Ward where for once her physical health can be properly assessed over a period of weeks. If the MH team stand in my daughter’s way of her physical health appointments and pathological tests I will report everything on here. I have already requested reports from all the professional bodies who have done nothing so far to stop the abuse to my daughter. Most importantly doctors should put the physical health of their patients first and foremost. I have now highlighted how patients are being deprived under just one area and how patients could have lost their lives due to the scans and how patients under the MH are refused pathological tests. This is why I was banned for months on end visiting my daughter and bullied by various doctors and this needs to be looked into. Police time has been wasted. Having lost close friends to cancer I intend to give this massive publicity.
LPFT under MH do not use PANSS??? Below is what I have written to Lincolnshire Partnership Trust as I am concerned for all the patients on Castle and Ellis Ward who may not have had reliable scans and I do not think anyone is being treated properly and wish to share so that everyone can be aware of the true facts:
PANSS
The PANSS score is an essential diagnostic tool which LPFT are not using and should be. All the scans may need to be re-done under scanners in Sheffield not just the MRI – everything and you may have to review all the patients on both Castle and Ellis Wards who have had scans done in Lincoln under the 1.5 Tesla in light of the revelations below.
The PANSS score is a long established test approved by the Royal College of Psychiatrists and used by NHS Mental Health Teams in many of the trusts to determine the severity of the schizophrenia the patient is suffering from. Its purpose is to confirm diagnosis, to guide the treatment regimen and to determine suitability for matters such as section 17 leave, suitability of the patient for post-discharge accommodation and eventual discharge from mental health care.
Here are LPFT’s comments below:
“LPFT does not use the PANSS scale for various reasons but does use the Glasgow Antipsychotic side effect scale (GASS). This measures the side effects of antipsychotics rather than the efficacy of antipsychotics”.
This is totally unsatisfactory for the following reasons. To begin with to quote LPFT’s own words “for various reasons” gives no explanation at all why this scale is not used by LPFT and is a cursory and unhelpful excuse.
The PANSS scale as mentioned above is crucial in determining not only treatment but deprivation of liberty and the ability of Elizabeth to enjoy leave and to have quality time off the ward. Elizabeth’s stifling detention without hope of even the chance to have a day out or to spend time with her family on important occasions like Christmas and her birthday are a contribution to her state of mind and a detriment to her eventual recovery.
The scale is also used to determine an appropriate treatment regimen which goes beyond the simple use or rapid tranquillisation and isolation preferred by the staff of the hospital in which she is detained. The hospital has obstructed all attempts to have Elizabeth’s mental health condition based on a determination that their ‘diagnosis ‘ of schizophrenia would be the only option. Elizabeth is now seeing a neurologist but that has only happened because that intervention was sought by me and was indeed actively discouraged and obstructed by the Responsible Clinician and the Clinical Lead on the ward.
The Glasgow Antipsychotic Side effect (GASS) scale that LPFT refer to in their email has an entirely different purpose to the PANSS scale and you are well aware of that. The GASS effect scale is for detecting adverse drug reactions and it has to be said if they are indeed using this they have ignored a number of these over the last two and a half years in spite of them being pointed out to them.
LPFT are fully aware that the GASS scale is not a substitute for PANSS but an entirely different test and the reply to the NR was disingenuous and unhelpful. To date no detailed explanation of why PANSS is not being used has been given and the Mental Health Act Team (notably the email does not identify its author) have failed to help once again. Please explain.
In the absence of proper monitoring by the people entrusted with Elizabeth’s care is it hardly surprising that after two and a half years subjected to a deprivation of liberty regime more restrictive than a section 37/41 order and constant prn rapid tranquillisation that she has made no improvement and is as far away from discharge as she ever has been.
The fact is the private scans are most certainly more superior to theirs and have been shown to numerous experts who are biomedical scientists yet they agree. If LPFT hadn’t spent a fortune getting rid of me as NR they would have more money to spend on decent scanners such as Tesla 3 and not having one is putting everyone’s life at risk not just those under MH. The taking away of my daughter’s right of capacity and autonomy is the biggest violation of all human rights. About 10 doctors apart from Dr Memons of Cygnet have stood in the way of her having MRI scans so that is why I was suspicious and arranged it myself. The MH system is ridiculous and I was the best NR and they got rid of me for their own convenience which again is abrogation of my daughter’s human rights. As highlighted in Medscape it is mentioned about brain tumours being missed and metastacising before being found which is potentially fatal which is why I am warning everyone not to trust their NHS scans and to check on which scanner has been used by their Trust.
It is also important to get brain lipids tested. They can affect both metabolising enzymes and result in ADRs. Several endocrine/metabolising disorders are associated with elevated levels of lipids (hyperlipidemia).
RESPONSIBLE CLINICIANS ARE SUPPOSED TO FOLLOW THE MHA 1983 BUT UNDER LPFT WHAT IS BEING DONE IS NOT CONDUCIVE TO ELIZABETH’S RECOVERY AND I WILL FEATURE MORE SHOCKING REVELATIONS ON MY NEXT BLOG. THEY NEEDED TO ROB HER OF HER CAPACITY SO THAT THEY COULD ABUSE THE CONCEPT OF THERAPEUTIC NECESSITY WHILST LABELLED WITH NO CAPACITY. I HAVE CAUGHT ON TO THEIR CRAFTINESS AS THIS GETS THEM OUT OF CONSULTING WITH HER OR RECORDING HER WISHES AND THIS IS WHY THEY GOT RID OF ME AS NR AND THIS IS TO PROTECT THEMSELVES. NO HUMAN RIGHTS AT ALL ARE TAKEN INTO ACCOUT BY LPFT. THE TERRIBLE DENIAL OF LIFE EXPERIENCE IS DETRIMENTAL TO MY DAUGHTER’S MENTAL AND PHYSICAL HEALTH AND TOTAL ABROGATION OF MEDICAL ETHICS. EVEN A S37/41 PATIENT IS NOT DENIED SUCH RIGHTS. HOW CAN HER DETENTION BE LAWFUL UNDER MHA 1983. THEY CONTINUALLY FLOUT THE STATUTORY SAFEGUARDS. THEY SHOULD BE SUBJECTED TO JUDICIAL REVIEW AND PROFESSIONAL MISCONDUCT ACTIONS.
Why 3T is necessary for detecting lesions
■ In more than 500 follow-up images, only four of 1996 new or enlarged multiple sclerosis lesions would have been missed with 3.0-T MRI without the administration of contrast material.
■ With 3.0-T MRI, the assessment of interval progression did not differ between contrast-enhanced and nonenhanced images.
Introduction
Inflammatory lesions in multiple sclerosis (MS) are detected as focal areas of high signal intensity on T2-weighted MR images. By depicting newly occurring lesions, MRI reveals subclinical disease activity. Therefore, regular follow-up MRI is considered a mainstay of clinical care for patients with MS or clinically isolated syndromes.
Earlier studies have reported that the administration of contrast material is necessary to maximize sensitivity for detecting new lesions. However, these results date back more than 2 decades and were based on two-dimensional images obtained with 4–5-mm-thick sections at magnetic field strengths of 1.5 T and lower.
MRI units with higher field strengths have become widely available, especially for brain imaging. In addition, three-dimensional isotropic MRI sequences were introduced and were shown to outperform conventional two-dimensional sequences in lesion depiction; they are therefore part of recommended MRI standards in MS . Furthermore, the double inversion-recovery (DIR) sequence was introduced. Although this sequence is best known for its ability to depict cortical lesions, it is also useful for depicting white matter lesions Recently, longitudinal subtraction techniques have been developed that show new or enlarged lesions as bright spots while pre-existing lesions and normal-appearing brain parenchyma are canceled out.* Such techniques substantially improve the sensitivity in the detection of new or enlarged lesions in MS at follow-up imaging.
We hypothesized that the use of contrast material does not improve sensitivity in the detection of new or enlarged lesions at follow-up MRI when modern three-dimensional sequences performed at a field strength of 3.0 T are used together with longitudinal subtraction maps. We therefore performed this study to investigate whether the use of contrast material has an effect on the detection of new or enlarged MS lesions and, consequently, the assessment of interval progression.
*The private 3T scans are much more able to see the lesions that the inappropriate 1.5T scanner cannot see.
The higher resolution scans cancel out the distortions and signal noise that hide the lesion and make the scan look normal.
1.5T MRI scanners are not fit for purpose in discovering brain lesions and inflammation.
Brain lesions and inflammation, especially in the temporal lobe are responsible for poor drug response and in some cases for diagnosis.
1.5T scans are responsible for false negative (normal) brain images.
Neuro Second Opinion Catches Missed Brain Lesions Suggestive of MS
American Roentgen Ray Society Dynamic contrast-enhanced MRI (DCE-MRI) has clearly been shown to be a highly sensitive tool for the detection of breast cancer [1–14]. Reported high sensitivity (83– 100%) [1–5] of MRI for breast cancer led im[1]agers initially to presume that non-enhancing legions on MRI were benign and did not warrant biopsy [1, 15]. However, subsequently reported articles have shown that all malignant lesions do not show enhancement at DCE[1]MRI [2, 5, 16–20], with enhancement absent in up to 12% of known malignant lesions. In a recent multi-institutional study of 995 lesions in 854 women, Schnall et al. [20] reported that 16% of 77 ductal carcinoma in situ (DCIS) lesions and 3% of 422 invasive cancers showed no enhancement. Teifke et al. [18] found 28 (8.4%) of 334 invasive cancers and 13 (65%) of 20 non-invasive cancers were missed at MRI. The reasons given for lack of visualization of these missed lesions were technical difficulties, reader percep[1]Keywords: breast cancer, DCE-MRI, dynamic contrast-enhanced MRI DOI:10.2214/AJR.09.3568 Received September 3, 2009; accepted after revision December 8, 2009.
R. A. Schmidt is a minor stockholder in Hologic Inc., and his spouse receives grant support from Philips Healthcare. G. M. Newstead receives grant support from Philips Healthcare, and her spouse is a minor stockholder in Hologic Inc. WOMEN ’ S I M A G I N G OBJECTIVE.
The objective of our study was to determine the sensitivity of cancer detection at breast MRI using current imaging techniques and to evaluate the characteristics of lesions with false-negative examinations. MATERIALS AND METHODS. Two hundred seventeen patients with 222 newly diagnosed breast cancers or highly suspicious breast lesions that were subsequently shown to be malignant underwent breast MRI examinations for staging. Two breast imaging radiologists performed a consensus review of the breast MRI examinations. The absence of perceptible contrast enhancement at the expected site was considered to be a false-negative MRI. Histology of all lesions was reviewed by an experienced breast pathologist. RESULTS. Enhancement was observed in 213 (95.9%) of the 222 cancer lesions. Of the nine lesions without visible enhancement, two lesions were excluded because the entire tumor had been excised at percutaneous biopsy performed before the MRI examination and no residual tumor was noted on the final histology. The overall sensitivity of MRI for the known cancers was 96.8% (213/220); for invasive cancer, 98.3% (176/179); and for ductal carcinoma in situ, 90.2% (37/41). CONCLUSION.
In a population of 220 sequentially diagnosed breast cancer lesions, we found seven (3.2%) MRI-occult cancers, fewer than seen in other published studies. Small tumor size and diffuse parenchymal enhancement were the principal reasons for these false[1]negative results. Although the overall sensitivity of cancer detection was high (96.8%), it should be emphasized that a negative MRI should not influence the management of a lesion that appears to be of concern on physical examination or on other imaging techniques. Shimauchi et al. MRI-Occult Breast Cancers Women’s Imaging Original Report Downloaded from ajronline.org by 90.246.25.176 on 02/27/24 from IP address 90.246.25.176. Copyright ARRS. For personal use only; all rights reserved AJR:194, June 2010 1675 MRI-Occult Breast Cancers stitution. Forty-four lesions in 44 patients were excluded because the final pathology at lumpectomy or mastectomy was performed at other institutions and was not available for review by our pathologists. The remaining 222 cancers in 217 patients were the subject of this retrospective review. The patients ranged in age from 28 to 85 years (median, 58 years). The spectrum of malignancy size and histology in these 217 patients is shown in Table 1. Of the 222 cancers studied, 84 (37.8%) lesions were palpable, 80 (36.0%) lesions were non-palpable, and clinical data as to palpability was not available for 57 (25.7%) lesions; 209 (94.1%) lesions were visible at mammography, 10 (4.5%) lesions were not visible at mammography, and mammograms were not available for three (1.4%) lesions. Additionally, 166 (74.8%) lesions were visible at sonography, 16 (7.2%) lesions were not visible at sonography, and ultrasound images were not available for 40 (18.0%) lesions. All index cancers, except 32 of 222 lesions, had been diagnosed by percutaneous biopsy or fine-needle aspiration (FNA) before MRI. The remaining 32 cancers underwent MRI because other imaging and clinical findings suggested a highly suspicious lesion and subsequent tissue sampling proved malignancy. Conventional Diagnostic Imaging In all but three patients, mammograms (obtained with different equipment and films, many from different referral centers) were available and were reviewed at our institution by breast imaging specialist radiologists before MRI. Mammograms obtained at outside referral centers accounted for approximately 20% of the total 217 patients. All patients with invasive cancer or extensive DCIS lesions (166 cases, 75%) underwent target[1]ed ultrasound examination of the affected breast and the ipsilateral axillary region, using an ATL HDI 5000 unit (Philips Healthcare International) and a 5-12–MHz linear transducer, before MRI. These imaging examinations were performed by breast specialist radiologists at our institution. An additional ultrasound examination was not standard procedure for patients with a diagnosis of pure DCIS at our institution unless mammograms showed extensive disease suspicious for the presence of an invasive component. MRI Protocol MRI examinations were performed using two 1.5-T imaging units (Signa, GE Healthcare, for 116 patients; and Intera Achieva, Philips Healthcare, for 101 patients). All patients underwent MRI in the prone position using parallel imaging technique. A dedicated 8-channel breast coil was used for the Signa scanner, and a dedicated 7-channel breast coil was used for the Intera Achieva scanner. After obtaining bilateral non-fat-saturated T2-weighted images (TR/TE: Signa, 5,000/103.5; Intera Achieva, 16,907/120) of the breasts, a T1-weighted 3D gradient-echo sequence was performed before and 20 seconds after the injection of contrast material. For the Signa scanner, the imaging parameters were as follows: 4.6/2.2; flip angle, 10°; field of view (FOV), 34 × 34 cm; matrix, 320 × 320; section thickness, 2 mm; and acquisition time, 75 sec[1]onds. For the Intera Achieva scanner, the parameters were as follows: 7.9/3.9; flip angle, 10°; FOV, 48 × 48 cm; matrix, 352 × 352; section thickness, 2 mm; and acquisition time, 75 seconds. A dynamic study in the axial plane was performed six times after initiation of an IV injection of 0.1 mmol/kg of gadodiamide (Omniscan, GE Healthcare) at a rate of 2 mL/s, which was followed by a 20-mL saline flush at the rate of 2 mL/s. MRI examinations were processed by CADstream, version 4.1 (Confirma), and subtraction images, time course curves, and angiogenesis maps were obtained. The images were transferred to a workstation (Advantage Windows, software version 4.0, GE Healthcare) for analysis. Image Analysis IRB-approved retrospective review by consensus was performed by two radiologists with expertise in breast MRI, one with 15 years’ experience and the other with 5 years. Images were interpreted with the benefit of a brief clinical history, knowledge of the histopathologic findings, and knowledge of the mammography and sonography results. In addition to the original images, maximum-intensity-projection and multiplanar reconstruction images were reviewed. The reviewers called findings positive even when there was no color on angiogenesis maps or when, for example, there was a persistent type of curve; they relied on morphology for diagnosis in these cases because TABLE 1: Pathologic Diagnosis in 217 Patients With 222 Malignancies Diagnosis No. (%) of Malignant Lesions No. (%) of Malignant Lesions by Size < 2 cm 2–5 cm > 5 cm Not Available Invasive ductal carcinoma 160 (72) 94 (80) 54 (76) 11 (55) 0 (0) Invasive lobular carcinoma 19 (8) 8 (7) 9 (13) 2 (10) 0 (0) Ductal carcinoma in situ 44 (20) 15 (13) 8 (11) 7 (35) 14 (100) Total 222 (100) 117 (100) 71 (100) 20 (100) 14 (100) TABLE 2: False-Negative Lesions at Dynamic Contrast-Enhanced MRI Case No. Patient Age (y) Pathology Imaging Reason for False[1]Type of Cancer Nuclear Grade Size (mm) Mammography Sonography Size (mm) Negative MRI 1 46 Extensive DCIS 2 NA Pleomorphic and linear calcifications NA 30 Diffuse parenchymal enhancement 2 43 DCIS 3 30 Pleomorphic calcifications Negative 25 Diffuse parenchymal enhancement 3 54 Multifocal DCIS 3 NA Punctate calcifications NA 5 Unknown 4 79 DCIS 1 5 Pleomorphic calcifications NA 5 Small size 5 53 IDC with DCIS 3 IDC, 0.8; DCIS, 10 Amorphous calcifications NA 10 Unknown 6 49 IDC with extensive DCIS 2 IDC, 8; DCIS, NA Pleomorphic and linear calcifications Hypoechoic masses 65 Diffuse parenchymal enhancement 7 44 IDC with DCIS 2 IDC, 12; DCIS, NA Negative Mixed echogenic mass 10 Unknown; low-signal mass on T2-weighted images Median 46 10 Note—DCIS = ductal carcinoma in situ, IDC = invasive ductal carcinoma, NA = not applicable. Downloaded from ajronline.org by 90.246.25.176 on 02/27/24 from IP address 90.246.25.176. Copyright ARRS. For personal use only; all rights reserved 1676 AJR:194, June 2010 Shimauchi et al. some malignant lesions especially DCIS and in[1]vasive lobular carcinoma (ILC) lesions can show slow uptake and perceptible kinetics [21, 22]. The absence of perceptive contrast enhancement at the expected site of the lesion was considered to be a false-negative MRI. Each study was also evaluat[1]ed with bilateral breast parenchymal enhancement scores of minimal, mild, moderate, or marked enhancement by consensus opinion. Technical factors such as patient motion, poor fat suppression, or susceptibility artifacts caused by percutaneously placed metallic clips did not compromise any of the study data sets. Histopathologic Correlation Of the 222 malignant cases, mastectomy was performed for 92 (41%) cases and breast-conserving surgery lumpectomy, with or without needle localization guidance, was performed for 130 cas[1]es (59%). Histology results of all lesions were re[1]viewed by an experienced breast pathologist with 25 years of experience in breast pathology. Tumor type, grade, size, and histologic subtype were documented in the pathology reports. In general, in our pathology department, extensive DCIS is defined as a lesion larger than 5 cm. Correlation between imaging and pathology for each case with regard to location and size and treatment management decisions were discussed for each case at weekly inter[1]nal multidisciplinary breast conference. Results Of the 222 cancerous lesions, enhancement was observed in 213 lesions (95.9%). There were nine examinations that showed no enhancement on MRI. All nine patients had undergone core biopsy or FNA before the MRI examination. Two of the nine lesions were excluded from our false-negative analysis, both presented with a cluster of calcifications, because the entire tumor had been excised by stereotactic core biopsy performed before the MRI examination. In these cases, no residu[1]al tumor was noted at histology on the sub[1]sequent excised breast specimens. Histology of both lesions indicated low-grade DCIS. The sensitivity of MRI for the known cancers was, therefore, 96.8% (213/220) for all cancer, 98.3% (176/179) for invasive cancer, and 90.2% (37/41) for DCIS. Of the 217 patients, 35 patients (16.1%) were recalled for MRI-directed ultrasound, 22 patients (10.1%) underwent ultrasound biopsies with benign results, and nine patients (4.1%) underwent MRI biopsies with benign results. The seven (3.2%) nonenhancing cancers included four cases of DCIS (one low-grade, one intermediate-grade, two high-grade), and three cases of invasive ductal carcinoma (IDC) (two intermediate-grade, one high-grade), as shown in Table 2. One of the two scanners was used for 116 patients (119 lesions), and four malignant lesions (3.4%) were missed. The other scanner was used for 101 patients (103 lesions), and three lesions (2.9%) were missed. All of the false-negative lesions except one were detected at mammography. The mammographic features of these lesions were classified as pleomorphic and linear calcifications (2/6), pleomorphic calcifica[1]tions (2/6), amorphous calcifications (1/6), and punctate calcifications (1/6). One lesion was detected as a palpable, tender mass in the retroareolar region and was visible at sonog[1]raphy but not at mammography. The overall A C Fig. 1—79-year-old woman with history of right lumpectomy for ductal carcinoma in situ (DCIS) 10 years earlier (case 4 in Table 2). A, Craniocaudal magnification view of right breast from routine follow-up mammography shows 5-mm cluster of pleomorphic calcifications (arrow) near lumpectomy scar. Stereotactic core biopsy revealed DCIS, grade 1. B, Craniocaudal mammographic view of right breast obtained after biopsy shows metallic clip with a few residual calcifications (arrow) at site of biopsy. C, T2-weighted image shows susceptibility artifact from metallic clip (arrow). D, On early phase of dynamic contrast-enhanced study (subtraction, T1-weighted image), no enhancement is seen around clip (arrow). Subsequent right mastectomy revealed DCIS measuring 5 mm in vicinity of biopsy site. B D Downloaded from ajronline.org by 90.246.25.176 on 02/27/24 from IP address 90.246.25.176. Copyright ARRS. For personal use only; all rights reserved AJR:194, June 2010 1677 MRI-Occult Breast Cancers median size of the false-negative lesions on final pathology evaluation was 10 mm. There were four false-negative DCIS lesions, one of which was very small by pa[1]thology (5 mm) (Fig. 1). Two other DCIS lesions were obscured by diffusely enhancing surrounding parenchyma (Fig. 2) even at the early phase (75 seconds) of the dynamic study. The remaining multifocal DCIS lesion (grade 3) did not show enhancement in a background of minimal parenchymal enhancement for reasons that are not known. There were three false-negative invasive carcinomas. One 8-mm IDC with extensive DCIS was obscured by diffusely enhancing surround[1]ing parenchyma (Fig. 3). One very small (0.8 mm) IDC with DCIS did not show enhancement in a background of mild parenchymal enhancement for reasons that are not known. The remaining lesion, IDC with DCIS, was visible on T2-weighted images as a low-signal mass; however, no enhancement was noted after the administration of contrast medium. Discussion In this study, DCE-MRI offered a high sensitivity in a cohort of patients with newly diagnosed breast cancer. Sensitivity for all breast carcinoma, invasive carcinoma, and in situ carcinoma was 96.8%, 98.3%, and 90.2%, respec[1]tively. These results are comparable or slightly superior to previously published results [18– 20] (Table 3). This improvement could be explained by the more modern technical parameters used compared with those of prior studies—that is, higher field strength (1.5 T), higher temporal resolution (75 seconds), and higher spatial resolution (slice thickness, 2 mm; in-plane resolution, 1–1.5 mm). The percentage of palpable lesions in this study (84/164 lesions, 51%), when known, was similar to or lower than the percentage of palpable findings in previously reported studies [7, 20]. However, there are some differences in study methodology when this experience is compared with prior reports [18, 20]. Entry criteria in these prior studies include patients with histologically proven benign lesions and those with malignant lesions. In contrast, the reported sensitivity in this study and in the study by Ghaiet al. [19], both retrospective studies, was achieved in cases in which readers knew malignancy was present before reading MRI studies. In the study by Schnall et al. [20], 13 (3.1%) of 422 invasive lesions and 12 (15.6%) of 77 DCIS lesions did not exhibit enhancement at MRI. Teifke et al. [18] found that 28 (8.4%) of 334 invasive lesions and 13 (65%) of 20 DCIS lesions were missed at MRI. In addition, unlike the cases presented in this report, the false-negative lesions described by Teifke et al. included malignancies that were not detected because of technical reasons. No technically inadequate examinations compromised this study and none were included in that of Ghai et al. Despite these differences in study design, the results of this study and all other studies show the existence of MRI-occult breast malignancies. In this study, seven cancers (3.2%) showed no enhancement on MRI. Of the seven false[1]negative cases, four malignancies represented pure DCIS. Pure DCIS lesions often present as nonmass, clumped enhancement in a segmental or linear distribution [23] with plateau or washout curve types [22–25] but with lower peak enhancement values. Non-mass-like enhancement may be more difficult to perceive TABLE 3: Data From Published Articles Compared With Data From This Study Journal, Year of Publication First Author [Reference No.] Total No. of Lesions No. of False-Negative Lesions Sensitivity (%) Total Invasive Cancer In Situ Cancer Total Invasive Cancer In Situ Cancer AJR, 2005 Ghai [19] 104 9 9 — 91.3 91.3 — Radiology, 2002 Teifke [18] 354 41 28 13 88.4 91.6 35.0 Radiology, 2006 Schnall [20] 995 25 13 12 95.0 96.9 84.4 This study 220 7 4 3 96.8 98.3 90.2 Note—Dash (—) indicates no ductal carcinoma in situ present in this population. A Fig. 2—43-year-old woman with screening-detected pleomorphic calcifications measuring 2.5 cm in right breast (case 2 in Table 2). Stereotactic core biopsy revealed ductal carcinoma in situ (DCIS), grade 3. A, Craniocaudal mammographic view of right breast obtained after stereotactic core biopsy shows residual calcifications (arrows). B, On early phase of dynamic contrast-enhanced study (subtraction, T1-weighted images), no abnormal enhancement is observed at area of susceptibility artifact from metallic clip placed after stereotactic core biopsy (arrow) because of diffuse parenchymal enhancement. Needle localization lumpectomy revealed DCIS, grade 3, measuring 3 cm. B Downloaded from ajronline.org by 90.246.25.176 on 02/27/24 from IP address 90.246.25.176. Copyright ARRS. For personal use only; all rights reserved 1678 AJR:194, June 2010 Shimauchi et al. especially in the presence of enhancing breast parenchyma. This observation is supported by a report from the MRI Lexicon Committee indicating that reader agreement for the classification of linear enhancement distribution was poor [24]. There were three cases (two DCIS and one IDC with DCIS) in patients who were younger than the median age of the patient cohort with diffusely enhancing surrounding parenchyma, that could obscure an abnormal enhancing lesion. The median age of these three patients was 46 years, whereas the median age of newly diagnosed cancer patients overall was 58 years. One limitation of this study is that we did not take the hormonal status of our patients into account for scheduling the examinations. At our institution, scheduling patients for breast MRI to stage newly diagnosed cancer has not routinely been done according to the phase in the menstrual cycle for premenopausal women. Perhaps imaging in the second week or at least in the middle of the menstrual cycle, as advocated by Viehweg et al. [26] and Müller-Schimpfle et al. [27], might reduce the number of cases with false-negative MRI due to diffusely enhancing surrounding parenchyma. However, this type of scheduling can be psychologically stressful for patients and can present a perceived delay in care. Of the remaining false-negative malignancies, one was a small (0.8 mm) IDC with DCIS. Teifke et al. [18] suggested that infiltrating cancers associated with DCIS might be difficult to detect on MRI. The sensitivity of MRI for DCIS reported by Teifke et al. was 35%, and those investigators concluded that MRI cannot reliably diagnose DCIS-positive cancers. Although there are some differences in the study methodologies in this study, the sensitivity for DCIS was 90.2%, which suggests that improvement in DCE-MRI technique may aid in achieving a higher sensitivity for DCIS. Further studies are required to prove a definitive association between false-negative MRI examinations and DCIS lesions. Other invasive cancers may not be visualized readily because of very small size or because of diffuse pattern of spread. Prior studies have shown ILC to be MRI occult because of diffuse infiltration without mass formation [16, 17, 19]. However, in this study, all ILC lesions (8.6% of total malignancies) were detected at MRI. The relatively thicker slice thickness (range, 3–10 mm) used in pri[1]or reported studies could have negatively impacted the sensitivity of MRI for ILC. A limitation of this study includes a possible bias because it is a retrospective review. At the time of the retrospective read for this study, re[1]viewers were aware of both the initial and the final histologic findings. In routine practice, we may not be aware of all of the details concerning the histology for all cases, although we routinely have histology or cytology findings for most staging MRI cases at the time of the prospective read. However, this study has shown that improved technical parameters— that is, a higher field strength (1.5 T), higher temporal resolution, higher spatial resolution, and improved coil design—led to better results for the detection of small malignant lesions, particularly DCIS. To summarize, in a population of 220 sequentially diagnosed known breast cancer lesions, we found seven (3.2%) MRI-occult cancers, which is fewer than reported in other published studies. Small tumor size and dif[1]fuse parenchymal enhancement were likely the principal reasons for these false-negative results. Although the overall sensitivity of breast MRI for cancer detection was high (96.8%), it should be emphasized that a negative MRI should not influence the management of a lesion that appears to be of concern on physical examination, mammography, or ultra[1]sound. MRI is complementary to—but is not a replacement for—other breast imaging techniques and should not be used as the sole imag[1]ing study because, as this study shows, a small number of cancers may not be visible at MRI. References 1. Harms SE, Flamig DP, Hesley KL, et al. MR imaging of the breast with rotating delivery of excitation off resonance: clinical experience with pathologic correlation. Radiology 1993; 187:493–501 2. Gilles R, Guinebretiere JM, Lucidarme O, et al. Nonpalpable breast tumors: diagnosis with contrast-enhanced subtraction dynamic MR imaging. Radiology 1994; 191:625–631 3. Kaiser WA. False-positive results in dynamic MR A Fig. 3—49-year-old woman with diffuse pleomorphic and linear calcifications measuring 6.5 cm in right breast, proven to be DCIS, grade 2, by stereotactic core biopsy (case 6 in Table 2). A, Mediolateral magnification view of right breast obtained after stereotactic core biopsy shows calcifications (arrows). Metallic clip (arrowhead) was placed in upper inner quadrant. B, On early phase of dynamic contrast-enhanced study (subtraction, T1-weighted images), no abnormal enhancement is observed in upper outer quadrant of right breast because of diffuse parenchymal enhancement. Right simple mastectomy revealed 8-mm invasive ductal carcinoma, grade 2, with extensive ductal carcinoma in situ. B Downloaded from ajronline.org by 90.246.25.176 on 02/27/24 from IP address 90.246.25.176. Copyright ARRS. For personal use only; all rights reserved AJR:194, June 2010 1679 MRI-Occult Breast Cancers mammography: causes, frequency, and methods to avoid. Magn Reson Imaging Clin N Am 1994; 2:539–555 4. Fobben ES, Rubin CZ, Kalisher L, Dembner AG, Selt[1]zer MH, Santoro EJ. Breast MR imaging with commercially available techniques: radiologic–pathologic correlation. Radiology 1995; 196:143–152 5. Bone B, Aspelin P, Bronge L, Isberg B, Perbeck L, Veress B. Sensitivity and specificity of MR mam[1]mography with histopathological correlation in 250 breasts. Acta Radiol 1996; 37:208–213 6. Liberman L, Morris EA, Dershaw DD, Abramson AF, Tan LK. MR imaging of the ipsilateral breast in women with percutaneously proven breast can[1]cer. AJR 2003; 180:901–910 7. Berg WA, Gutierrez L, NessAiver MS, et al. Diag[1]nostic accuracy of mammography, clinical exami[1]nation, US, and MR imaging in preoperative as[1]sessment of breast cancer. Radiology 2004; 233:830–849 8. Sardanelli F, Giuseppetti GM, Panizza P, et al. Sensitivity of MRI versus mammography for detecting foci of multifocal, multicentric breast cancer in fatty and dense breasts using the whole[1]breast pathologic examination as a gold standard. AJR 2004; 183:1149–1157 9. Schnall MD, Blume J, Bluemke DA, et al. MRI detection of distinct incidental cancer in women with primary breast cancer studied in IBMC 6883. J Surg Oncol 2005; 92:32–38 10. Hollingsworth AB, Stough RG. Preoperative breast MRI for locoregional staging. J Okla State Med Assoc 2006; 99:505–515 11. Bilimoria KY, Cambic A, Hansen NM, Bethke KP. Evaluating the impact of preoperative breast magnetic resonance imaging on the surgical management of newly diagnosed breast cancers. Arch Surg 2007; 142:441–445; discussion, 445–447 12. Lehman CD, Gatsonis C, Kuhl CK, et al. MRI evaluation of the contralateral breast in women with recently diagnosed breast cancer. N Engl J Med 2007; 356:1295–1303 13. Van Goethem M, Schelfout K, Kersschot E, et al. MR mammography is useful in the preoperative locoregional staging of breast carcinomas with extensive intraductal component. Eur J Radiol 2007; 62:273–282 14. Braun M, Polcher M, Schrading S, et al. Influence of preoperative MRI on the surgical management of patients with operable breast cancer. Breast Cancer Res Treat 2008; 111:179–187 15. Kaiser WA. MR mammography [in German]. Ra[1]diologe 1993; 33:292–299 16. Boetes C, Strijk SP, Holland R, Barentsz JO, Van Der Sluis RF, Ruijs JH. False-negative MR imag[1]ing of malignant breast tumors. Eur Radiol 1997; 7:1231–1234 17. Wurdinger S, Kamprath S, Eschrich D, Schneider A, Kaiser WA. False-negative findings of malig[1]nant breast lesions on preoperative magnetic reso[1]nance mammography. Breast 2001; 10:131–139 18. Teifke A, Hlawatsch A, Beier T, et al. Undetected malignancies of the breast: dynamic contrast-en[1]hanced MR imaging at 1.0 T. Radiology 2002; 224:881–888 19. Ghai S, Muradali D, Bukhanov K, Kulkarni S. Nonenhancing breast malignancies on MRI: sonographic and pathologic correlation. AJR 2005; 185:481–487 20. Schnall MD, Blume J, Bluemke DA, et al. Diag[1]nostic architectural and dynamic features at breast MR imaging: multicenter study. Radiology 2006; 238:42–53 21. Van Goethem M, Schelfout K, Kersschot E, et al. Comparison of MRI features of different grades of DCIS and invasive carcinoma of the breast. JBR-BTR 2005; 88:225–232 22. Jansen SA, Newstead GM, Abe H, Shimauchi A, Schmidt RA, Karczmar GS. Pure ductal carcino[1]ma in situ: kinetic and morphologic MR charac[1]teristics compared with mammographic appear[1]ance and nuclear grade. Radiology 2007; 245:684–691 23. Shiraishi A, Kurosaki Y, Maehara T, Suzuki M, Kurosumi M. Extension of ductal carcinoma in situ: histopathological association with MR imag[1]ing and mammography. Magn Reson Med Sci 2003; 2:159–163 24. Ikeda DM, Hylton NM, Kinkel K, et al. Develop[1]ment, standardization, and testing of a lexicon for reporting contrast-enhanced breast magnetic res[1]onance imaging studies. J Magn Reson Imaging 2001; 13:889–895 25. Menell JH, Morris EA, Dershaw DD, Abramson AF, Brogi E, Liberman L. Determination of the presence and extent of pure ductal carcinoma in situ by mammography and magnetic resonance imaging. Breast J 2005; 11:382–390 26. Viehweg P, Paprosch I, Strassinopoulou M, Hey[1]wang-Köbrunner SH. Contrast-enhanced magnetic resonance imaging of the breast: interpreta[1]tion guidelines. Top Magn Reson Imaging 1998; 9:17–43 27. Müller-Schimpfle M, Ohmenhaüser K, Stoll P, Dietz K, Claussen CD. Menstrual cycle and age: influence on parenchymal contrast medium enhancement in MR imaging of the breast. Radiology 1997; 203:145–
Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA Woo-Suk Chung, M.D.1 , Tae-Sub Chung, M.D.1 , Hyung Jung Kim, M.D.2 , Chul Min Ahn, M.D.2 , Jae Hoon Lee, M.D.1 , Jin Hur, M.D.1 , Arthur Eung-Hyuck Cho, M.D.1 Purpose : Early detection of small brain metastases is important. The purpose of this study was to compare the detectability of brain metastases according to the size between 1.5 T and 3.0 T MRI. Materials and Methods : We reviewed 162 patients with primary lung cancer who were examined for TNM staging. After administration of double dose of Gd-DTPA, MR imaging was performed with SPGR by 3.0 T MRI and then with T1 SE sequence by 1.5 T MRI. In each patient, three readers performed qualitative assessment. Sensitivity, positive predictive value, and diagnostic accuracy were calculated in 3.0 T and 1.5 T MRI according to size. Using the signal intensity (SI) measurements between the metastatic nodules and adjacent tissue, nodule-to-adjacent tissue SI ratio was calculated. Results : Thirty-one of 162 patients had apparent metastatic nodules in the brain at either 1.5 T or 3.0 T MR imaging. 143 nodules were detected in 3.0 T MRI, whereas 137 nodules were detected at 1.5 T MRI. Six nodules, only detected in 3.0 T MRI, were smaller than 3.0 mm in dimension. Sensitivity, positive predictive value, and diagnostic accuracy in 3.0 T MRI were 100 %, 100 %, and 100 % respectively, and in 1.5 T MRI were 95.8 %, 88.3 %, and 85.1 % respectively. SI ratio was significantly higher in the 3.0 T MRI than 1.5 T MRI (p=0.025). Conclusion : True positive rate of 3.0 T MRI with Gd-DTPA was superior to 1.5 T MRI with Gd-DTPA in detection of metastatic nodules smaller than 3.0 mm. Index words :Magnetic resonance (MR), high-field-strength imaging Brain neoplasm, metastases Contrast medium Introduction Brain metastases present a poor prognosis suggesting a shortened survival time. Early diagnosis of brain involvement and determination of the number of metastases are important not only for quality of life but also for cost effectiveness (1-3). The decision regarding a conservative versus a surgical approach depends on the number of brain metastases detected by radiologic means (1-3). A contrast-enhanced MRI has become the method of choice for visualization of brain metastases (1). Highdose gadolinium-enhanced MR examinations may have advantages over 0.1 mmol/kg examinations in detecting early and/or small metastases (3-7). A delayed study can also increase the contrast (2). Comparing to the 1.5 T MRI with an axial T1-weighted spin echo sequence (SE), the higher field strength MR systems combined with a sequence of SPGR (spoiled gradient recalled acquisition in the steady state) and administration of a high dose of Gd-DTPA (gadopentetate dimeglumine) may also have advantages in detecting small metastases, although this has not yet been verified by clinical data. The purpose of this study is to compare the detectability of brain metastases classified according to the size of nodules, between thin slice SPGR of 3.0 T and conventional thick slice SE of 1.5 T MRI with the administration of a double dose of GdDTPA. Materials and Methods Patients From December 2002 to February 2004, a total of 162 consecutive patients with primary lung cancer participated in our study. The institutional review board approved our study, and informed consent was obtained from all patients regarding the potential risks of both the double dose of contrast medium and two assessments by MRI scanning on a 3.0 T and 1.5 T machine. After the study, 31 patients of this population were diagnosed as having brain metastases. Mean patient age was 61.2 (range, 43 to 80 years). Protocol On the 3.0 T MR scanner (GE Signa VH/i; GE medical system, Milwaukee, USA), the images were acquired using a standard head coil and an actively shielded gradient system with a maximum gradient strength of 43 mT/m. On the 1.5 T MR scanner (Magnetom Vision; Siemens Medical Systems, Erlangen, Germany), a standard head coil and a maximum gradient strength of 25 mT/m were used. All patients were examined after administrating a contrast agent with a double dose of Gd-DTPA (0.2 mmol/kg). First, examinations were performed on a 3.0 T MR scanner and then were subsequently performed on a 1.5 T MR scanner without additional contrast injection. The scan interval between the 3.0 T and 1.5 T MR examination was less than 20 minutes. The contrast agent used was Gd-DTPA (Magnevist; Schering AG, Berlin, Germany). In all patients, the double dose of Gd-DTPA at 0.2 mmol/kg was administered intravenously as a bolus and scanning commenced immediately. MR imaging included the following sequences on both scanners: At 3.0 T MRI, an axial 3D SPGR, which is usually used at present, was used (TR/TE/TI = 5.7/1.44/400 milliseconds; flip angle 20°; 2 mm slice thickness; FOV of 220 mm; matrix size of 512×512 ZIP; spatial resolution of 0.43×0.43×2 mm; two acquisition) with a scan time of 3 minutes 30 seconds. At 1.5 T MRI, an axial T1-weighted spin echo sequence was used (TR/RE = 600/14 milliseconds; flip angle 90°; 5 mm slice thickness; FOV of 210 mm; matrix size of 174×256; spatial resolution of 1.2×0.82×5 mm; two acquisition) with a scan time of 5 minutes 30 seconds. Three radiologists performed randomized, independent blinded review. The three readers were merely informed that all of the patients had lung malignancies. The postcontrast MR examinations of the brain on all of the patients were evaluated. The readers did not have access to other image sets within each study. The presence, size, and number of metastatic nodules were assessed. The postcontrast images were divided into the following two groups: 3.0 T MRI with a double dose of Gd-DTPA and 1.5 T MRI with a double dose of Gd-DTPA. The readers were asked to document the number of nodules. Each nodule in each study was numbered and classified according to its largest diameter measurement: ≤3 mm, 3 mm to 5 mm, or 5 mm. Woo-Suk Chung et al
102 – Subsequently, if there was any debate about nodule classification, a final interpretation using imaging studies was done until consensus among the readers was accomplished. If disagreements persisted, 3-6 months of follow-up MR scans were obtained for further validation. For the patients who had follow-up MR scans, these scans were considered positive for metastases if there was a response to the treatment or if there was a growth of nodules identified during the follow-up period. In addition, the sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of the 3.0 T and 1.5 T MRI were calculated using the results from the final interpretation according to size. A quantitative image assessment was performed next. The same lesions on scans of the two different MRI systems were determined by comparing peripheral structures. Signal intensities of adjacent tissue and nodule were assessed by region of interest (ROI) measurements placed identically on both series of images using the same sized circular ROI from the software available on both scanners. Nodule-toadjacent tissue contrast (SI ratio) is defined by SI ratio = ×100 Stissue1 taken as the signal intensity of an ROI assessed over a nodule and Stissue2 taken as the signal intensity assessed over the contralateral white matter. The signal intensity of a nodule was measured within an enhanced area. In inhomogeneously enhanced nodules, the area of maximum uptake was chosen for measurement. Statistical Analysis The paired Wilcoxon’s signed ranks test was used to compare qualitative scores, and the matched-pair-t test was used to compare nodule SI ratios between the 3.0 T and 1.5 T MRI with a double dose of Gd-DTPA. For all tests, significance was set at p < 0.05, and SPSS software (SPSS Inc. Chicago, US) was used for statistical analyses. Results In the final review made by consensus of three radiologists (Table 1), a total of 143 metastatic nodules were detected by the 3.0 T MRI with a double dose of Gd-DTPA. Of these nodules, 49 nodules were ≤ 3 mm in diameter, 37 nodules were 3 mm to 5 mm, and 57 nodules were >5 mm. A total of 137 metastatic nodules were detected by the 1.5 T MRI with a double dose of Gd-DTPA in the final interpretation. Of these nodules, 43 nodules were ≤ 3 mm in diameter. The 3.0 T MRI with a double dose of Gd-DTPA was significantly more effective at detecting nodules smaller than 3 mm (p = 0.014) than the 1.5 T MRI. However, we found no significant difference in the detection of nodules larger than 3 mm (p > 0.05) (Table 1). In 6 of the 31 cases, six nodules, which were only detected by the 3.0 T MRI with a double dose of GdDTPA, and missed by the 1.5 T MRI with a double dose of Gd-DTPA, were unanimously agreed upon by all participants in the final interpretation. In three of the six nodules, a growing nodule was detected during a follow-up MR scan which confirmed the presence of metastases (Fig. 1). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of Gd-DTPA due to artifact (Fig. 2). Finally the 3.0 T MRI with a double dose of Gd-DTPA was Stissue1 – Stissue2 Stissue2 Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA
103 – Table 1. Total Number of Brain Metastases Classified by Size and Detected at the Final Interpretation Size 3.0 T MRI with 1.5 T MRI with p value Gd-DTPA Gd-DPTA ≤ 3 mm 49 43 0.014 3 mm<-≤5 mm 37 37 > 0.05 5 mm< 57 57 > 0.05 Total 143 137 0.014 Note : Data are the number of nodules Table 2. The Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRIs with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm Present Absent Present Absent 3.0 T MRI with Positive 143 00* 49 0* Gd-DTPA Negatiive 000 00* 00 0* 1.5 T MRI with Positive 137 18* 43 18* Gd-DTPA Negative 006 00* 06 0*
Pseudolesions that were detected as nodules by the 1.5 T MRI were detected as vascular structures by the 3.0 T MRI. useful for confirming the presence of these nodules. Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter or better delineation than by the 1.5 T MRI with a double dose of Gd-DTPA. Out of 137 nodules, 65 were brighter (Fig. 3) and out of 137 nodules, 63 were better delineated (Fig. 4). Fortyfive of 137 nodules were satisfactory in both conditions. By consensus, the final review stated, nodules detected by the 3.0 T and 1.5 T MRI were considered positive for metastases (Table 2). Additionally, there were 18 pseudolesions which were detected as nodules by the 1.5 T MRI, but as vascular structures by the 3.0 T MRI (Fig. 5). The sensitivity, positive predictive values, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 95.8%, 88.3%, and 85.1% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of the 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and Woo-Suk Chung et al
104 – a b Fig. 2. A 73-year-old male with multiple brain metastases. Metastatic nodule (a) by a 3.0 T MR image with a double dose of Gd-DTPA show a metastatic nodule (arrow). But (b) the 1.5 T MR image with a double dose of Gd-DTPA cannot show the metastatic nodule by artifact. abc Fig. 1. A 65-year-old male with single brain metastasis. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a small metastatic nodule (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA cannot show the nodule. In (c), a growing nodule was detected during the follow-up MRI with a double dose of Gd-DTPA which confirmed the presence of metastasis (arrow). 100% respectively. For metastatic nodules smaller than 3 mm, the sensitivity, positive predictive value, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 87.8%, 70.5%, and 64.2% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and 100% respectively (Table 3). For quantitative image assessment, the SI ratio in the post contrast sequences (Table 4) was significantly higher in the 3.0 T MRI with a double dose of GdDTPA than in the 1.5 T MRI with a double dose of GdDTPA (p = 0.025). Discussion Detection of metastatic nodules is dependent on both their size and contrast ratio (2). As methods to increase the contrast, a higher dose of Gd-DTPA, a higher field strength, and delayed study can all be used to aid detection (2-5, 8-17). Nodules larger than 10 mm are easily detected because vasogenic edema is customarily associated with larger metastases (2). So, when a higher dose of Gd-DTPA is used, the detection rate of larger nodules is not influenced. However, a higher dose is helpful for detecting small nodules because it increases nodule enhancement, yet this method has the disadvantages of increasing the false positive rate and promoting side effects (2-5, 8-14). A delayed study can also increase the contrast (2). It has been recommended that image acquisition be delayed from 5 to 35 minutes after the administration of contrast material at a dose of 0.1 mmol/kg to ensure optimal detection (2, 15). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of GdDTPA due to partial volume artifact. Eighteen lesions were detected in the 1.5 T MRI with a double dose of Gd-DTPA, which proved to be vascular structures in 3.0 T MRI with a double dose of Gd- DTPA. The true nature of these lesions was revealed because of the greater morphologic detail visualized by the high field Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA
105 – a b Fig. 3. A 65-year-old male with multiple brain metastases. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhancement (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhancement (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter than when observed by the 1.5 T MRI with a double dose of GdDTPA. Table 3. Estimation of the Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRI with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm 3.0 T 1.5T 3.0 T 1.5T Sensitivity 100 95.8 100 87.8 Specificity – 0 – 0 Positive predictive value 100 88.3 100 70.5 Negative predictive value – 0 – 0 Diagnostic accuracy 100 85.1 100 64.2 Table 4. Results of a quantitative assessment of nodules that were detected by the 3.0 T and 1.5 T MRIs with Gd-DTPA (n=137) 3.0 T 1.5 T P value Nodules-to-adjacent tissue: SI ratio 94.59 63.86 0.025 strength MR image, thus allowing differentiation between true enhancing lesions and sulcal vessels. In our study, each nodules was classified according to its largest diameter as being ≤ 3 mm, 3 mm to 5 mm, and >5 mm because the slice thickness of the 3.0 T MRI was 2.0 mm and 5 mm for the 1.5 T MRI. Therefore this study classified small metastatic nodules as being smaller than 3 mm. Although our study supports the use of a higher field strength MRI with a double dose of Gd-DTPA for increased metastatic nodule detection and for improved nodule enhancement and delineation, the results should be interpretated with caution. The reason for this is that for patients with two or more brain metastases, additional metastases found with the 3.0 T MRI seem to be of limited clinical importance. The presence of two or more small nodules generally will not change the way the patient is managed. Therefore, it is of utmost importance to identify the difference between none, one, and more than one metastatic nodule. Patients with a single metastatic nodule located in a respectable region can be treated surgically, and the tumor staged as M1, not M0. However, patients with two or more metastatic nodules are usually Woo-Suk Chung et al
106 – a b Fig. 5. A 67-year-old female with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows vascular structure (arrow). (b) The 1.5 T MRI with a double dose of GdDTPA shows a nodular lesion (arrow). A pseudolesion that was detected as a nodule by the 1.5 T MRI with a double dose of GdDTPA but as a vascular structure by the 3.0 T MRI with a double dose of Gd-DTPA is showed in this figure. a b Fig. 4. A 64-year-old male with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows a metastatic nodule with ring enhancement (arrow). (b) The 1.5 T MRI with Gd-DTPA show a metastatic nodule with ring enhancement (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were better delineated than when observed by the 1.5 T MRI with a double dose of GdDTPA. treated with radiation therapy and/or systemic chemotherapy (3, 18-22). On the other hand, the use of a higher strength field MRI was found to be helpful in confirming the appearance of an equivocal metastatic nodule. The 3.0 T MRI with a double dose of Gd-DTPA was also useful for the detection of additional metastases in patients with a known lesion detected by the 1.5 T MRI with a double dose of GdDTPA. Because this also has influence on the sensitivity, positive predictive value, and diagnostic accuracy the 3.0 T MRI with a double dose of GdDTPA was found to have better results than the 1.5 T MRI with a double dose of Gd-DTPA in our study. Therefore we recommend the use of the 3.0 T MRI with a double dose of Gd-DTPA in only three circumstances: when the findings by the 1.5 T MRI with Gd-DTPA are equivocal, when one potentially surgically respectable nodule is identified, or for detecting early and/or small metastases There were two limitations in this study. The first limitation was a difference in protocol sequence. The T1 weighted spin-echo protocol was used for the 1.5 T MRI and SPGR technique protocol for the 3.0 T MRI. Detectability of metastatic nodules is more effective with 3.0 T MRI with T1 SE than with a 1.5 T MRI with SE (2). SPGR with thin slice thickness is superior to the T1 spin echo sequence with thick slice thickness due to a partial volume effect. Additionally, SE is not optimum for a 3.0 T due to longer T1- and shorter T2- relaxation times of water protons, which decrease the contrast ratio in the 3.0 T images.17 The purpose of this study was to detect early small brain metastases, so using the SPGR sequence with a 3.0 T MRI, which is usually used at present, has advantages for detecting early small brain metastases. The second limitation was that the scan interval between the 1.5 T and 3.0 T MRI was less than 20 minutes. However, a delayed study increases contrast as mentioned above. The current study found that the SI ratio was significantly higher in the 3.0T images than in the 1.5 T images. Considering the delayed study by the 1.5 T MRI, this limitation emphasizes the better detection rate of the 3.0 T MRI with a double dose of Gd-DTPA. And due to these confounding variables, blinded reviews were performed by three readers. The detectability of metastatic nodules smaller than 3mm was better using a 3.0 T MRI with SPGR than a 1.5 T MRI with T1 SE. Therefore we recommend a 3.0 T MRI with SPGR and a double dose of Gd-DTPA for detecting early and/or small metastatic nodules, furthermore influencing treatment. References 1.Lassman AB, DeAngelis LM. Brain metastases. Neurol Clin. 2003; 21:1-23, vii, Review 2.Ba-Ssalamah A, Nobauer-Huhmann IM, Pinker K, et al. Effect of contrast dose and field strength in the magnetic resonance detection of brain metastases. Invest Radiol 2003; 38: 415-422 3.Sze G, Johnson C, Kawamura Y, et al. Comparison of singleand triple-dose contrast material in the MR screening of brain metastases. AJNR Am J Neuroradiol 1998; 19:821-828 4.Runge VM, Kirsch JE, Burke VJ, et al. High-dose Gadoteridol in MR imaging of intracranial neoplasm. J Magn Reson Imaging 1992; 2:9-18 5.Yuh WT, Engelken JD, Muhonen MG, Mayr NA, Fisher DJ, Ehrhardt JC. Experience with high-dose gadolinium MR imaging in the evaluation of brain metastases. AJNR Am J Neuroradiol 1992; 13:335-345 6.Brekenfeld C, Foert E, Hundt W, Kenn W, Lodeann KP, Gehl HB. Enhancement of cerebral diseases: How much contrast agent is enough? Comparison of 0.1, 0.2, and 0.3 mmol/kg Gadoteridol at 0.2 T with 0.1 mmol/kg Gadoteridol at 1.5 T. Invest Radiol 2001; 36:266-275 7.Yuh WT, Tali ET, Nguyen HD, Simonson TM, Mayr NA, Fisher DJ. The effect of contrast dose, imaging time, and lesion size in the MR detection of intracerebral metastasis. AJNR Am J Neuroradiol 1998; 16:373-380 8.Van Dijk P, Sijens PE, Schmitz PI, Oudkerk M. Gd-enhanced MR imaging of brain metastases: contrast as a function of dose and lesion size. Magn Reson Imaging 1997; 15:535-541 9.Yuh WT, Fisher DJ, Engelken JD, et al. MR evaluation of CNS tumors: dose comparison study with gadopentetate dimeglumine and gadoteridol. Radiology 1991; 180:485-491 10.Healy ME, Hasselink JR, Press GA, Middleton MS. Increased detection of intracranial metastases with intravenous GdDTPA. Radiology 1987; 165:619-624 11.Akeson P, Vikhoff B, Stahlberg F, Holtas S. Brain lesion contrast in MR imaging: dependence of field strength and concentration of gadodiamide injection in patients and phantoms. Acta Radiol 1977; 38:14-18 12.Runge VM. A review of contrast media research in 1999 –
Invest Radiol 2001; 36:123-130 13.Yuh WT, Parker JR Carvlin MJ. Indication related dosing for magnetic resonance contrast media. Eur Radiol 1977; 7(suppl 5):S269-S275 14.Rinck PA, Muller RN. Field strength and dose dependence of contrast enhancement by Gadolinium-based MR contrast agents. Eur Radiol 1999; 9:998-1004 15.Schorner W, Laniado M, Niendorf HP, Schubert C, Felix R. Time-dependent changes in image contrast in brain tumors after gadolinium-DTPA. AJNR Am J Neuroradiol 1986; Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA
107 – 7:1013-1020 16.Chang KH, Ra DG, Han MH, Cha SH, Kim HD, Han MC. Contrast enhancement of brain tumors at different MR field strengths: comparison of 0.5 T and 2.0 T. AJNR Am J Neuroradiol 1994; 15:1413-1419 17.Nobauer-Huhmann IM, Ba-Ssalamah A, Mlynarik V, et al. Magnetic resonance imaging contrast enhancement of brain tumors at 3 tesla versus 1.5 tesla. Invest Radiol 2002; 37:114- 119 18.Galicich JH, Sundaresan N, Thaler HT. Surgical treatment of single brain metastasis: evaluation of results by computerized tomography scanning. J Neurosurg 1980; 53:63-67 19.Runge VM, Carollo BR, Wolf CR, Nelson KL, Gelblum DY. Gd-DTPA: A review of clinical indications in central nervous system magnetic resonance imaging. Radiographics 1989; 9:929-958 20.Earnest F 4th, Ryu JH, Miller GM, et al. Suspected non-small cell lung cancer: Incidence of occult brain and skeletal metastases and effectiveness of imaging for detection-Pilot study. Radiology 1999; 211:137-145 21.Koutras AK, Marangos M, Kourelis T, et al. Surgical management of cerebral metastases from non-small cell lung cancer. Tumori 2003; 89:292-297 22.Soffietti R, Ruda R, Mutani R. Management of brain metastases. J Neurol 2002; 249:1357-1369. Review Woo-Suk Chung et al
108 – 통신저자 : 정태섭, 서울특별시 강남구 도곡동 146-92 연세대학교 영동세브란스병원 영상의학과 Tel. 82-2019-3514 Fax. 82-3462-5472 E-mail: tschung@yumc.yonsei.ac.kr 뇌전이종양의발견에있어서Doble dose Gd-DTPA를이용한 3 T MRI와1.5 T MRI간의비교연구 1 연세대학교 영동세브란스병원 영상의학과 2 연세대학교 영동세브란스병원 호흡기내과 정우석1 ·정태섭1 ·김형중2 ·안철민2 ·이재훈1 ·허 진1 ·조응혁1 목적: 작은 뇌전이 종양의 조기 발견은 중요하다. 이 연구의 목적은 1.5 T MRI와 3.0 T MRI 간의 크기에 따른 뇌 전이 종양의 발견율을 비교하는 것이다. 대상 및 방법: 폐암으로 진단 받은 162명의 환자를 대상으로 TNM 병기를 위해 뇌 MRI를 시행하였다. Gd-DTPA 를 2배 용량으로 투여 후, 3.0 T MRI에서 훼손경사회복획득으로 촬영하였으며 그 후 1.5 T MRI에서 T1 스핀 에 코로 촬영하였다. 3명의 방사선과 전문의가 합의하여 MRI를 판독하였으며 정성 평가를 시행하였다. 3.0 T와 1.5 T MRI에서 크기에 따라 민감도, 양성 예측률, 정확도를 평가하였다. 신호 강도를 사용하여 전이 종양과 인접 조직간 의 신호강도 비를 계산하였다. 결과: 162명의 환자 중 31명에서 1.5 T 또는 3.0 T MR에 뇌전이 종양이 발견되었다. 3.0 T MRI에서 143개의 종 양이 발견되었으나 1.5 T MRI에서 137개의 종양이 발견되었다. 6개의 종양이 3.0 T MRI에서만 발견되었으며 크 기는 모두 3 mm 미만이었다. 3.0 T MRI의 민감도, 양성 예측률, 정확도는 각각 100%, 100%, 100%이며, 1.5 T MRI에서는 각각 95.8%, 88.3%, 85.1% 이다. SI ratio는 1.5 T MRI보다 3.0 T MRI에서 유의하게 높았다 (p=0.025). 결론: Double dose Gd-DTPA를 이용한 3.0 T MRI는 3 mm미만의 뇌전이 종양을 발견하는데 있어서 1.5 T MRI 보다 우수하다.
4/16/20
Malcolm’s brain MRI was initially read as completely normal. Upon getting a second opinion, it was discovered that 22 lesions suggestive of multiple sclerosis had been missed. Here is his story.
[Malcolm] After 18 months of deteriorating health, with a multitude of neurological symptoms, I went to see a neurologist. I was ordered a standard brain MRI to help figure out what was going on. By this time, I had been researching my symptoms for a few months, and, in doing so, had developed a basic understanding of what I was looking for: T2 lesions.
When I received the results from my MRI, the report said everything was normal. I met with my neurologist, and he too said there was nothing abnormal about my scan. When I viewed the MRI myself, however, I found 4 spots that looked to me to be brain lesions. I brought them up to my doctor at my next appointment but was essentially laughed at.
It was quite unsettling to have something so concerning be shrugged off. After that appointment, I decided I wanted to switch to a new neurologist and get a second opinion on my MRI scan. I made an appointment with the new doctor, but it was going to be another 6 weeks before I could be seen. Fortunately, I found DocPanel. I submitted my MRI for review and, within 48 hours, I got my results back.
[Dr. Michael Rozenfeld] Malcolm reached out to DocPanel due to concern for a missed diagnosis. He was reportedly having symptoms suspicious for multiple sclerosis but his MRI was initially read as completely normal. Based on my review of his MRI, the exam was not normal. Malcolm had significant findings that were certainly suggestive of, but not entirely specific for, multiple sclerosis.
[Malcolm] My second opinion results were quite alarming – there were not 4 lesions, but 22. Twenty-two! They were small, but they were most definitely there. I took the second opinion report to my new neurologist, and now I am being considered for possible Primary Progressive Multiple Sclerosis. I am scheduled to get new MRIs in November to confirm or rule out MS and you can be sure I will be sending them to DocPanel for a second look!
I have found that the most important thing people in my shoes can do is be your own advocate. MS is such an odd and individual disease. – Malcolm
[Dr. Michael Rozenfeld] Radiology exams can be misinterpreted for a number of reasons – this is unfortunately not uncommon. While MRI is not the only piece in the puzzle for MS diagnosis, it plays a significant role. A false negative diagnosis made off an MRI scan could lead the neurologist and patient down an incorrect path and delay an accurate diagnosis, or potentially miss it entirely.
While MRI is not the only piece in the puzzle for MS diagnosis, it plays a significant role. A false negative diagnosis made off an MRI scan could lead the neurologist and patient down an incorrect path and delay an accurate diagnosis, or potentially miss it entirely.
The positive findings on Malcolm’s exam and his new report provide additional essential information for his neurologist, allowing him (the neurologist) to combine these imaging findings with other test results and physical exam findings to come to an accurate diagnosis.
I would always suggest patients seek a second opinion for complex medical diagnoses, especially if the patient feels that something is being missed or that their concerns aren’t being addressed. This could mean setting up an appointment with a second neurologist or submitting your radiology exams for a second opinion to a company such as DocPanel, where they will be interpreted by subspecialty trained and certified neuroradiologists. I personally like to explain the imaging findings in layman’s terms, to ensure that the patient understands the disease process. I believe this empowers patients so that they can take an active role in ensuring the best decisions regarding their care are made.
[Malcolm] After a few months of working with my current neurologist and a support group of people diagnosed with MS, I have found that the most important thing people in my shoes can do is be your own advocate. MS is such an odd, and individual disease. No two patients are exactly alike in their presentation or their symptoms. This can make it very difficult to diagnose. It is always helpful to get several opinions; your health is just to darn important.
DocPanel is committed to making sure every patient receives excellent care. If you would like an expert second opinion on your medical imaging scan from Dr.Rozenfeld or one of our other neuroradiology subspecialists, you can learn morehere.
Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA Woo-Suk Chung, M.D.1 , Tae-Sub Chung, M.D.1 , Hyung Jung Kim, M.D.2 , Chul Min Ahn, M.D.2 , Jae Hoon Lee, M.D.1 , Jin Hur, M.D.1 , Arthur Eung-Hyuck Cho, M.D.1 Purpose : Early detection of small brain metastases is important.
The purpose of this study was to compare the detectability of brain metastases according to the size between 1.5 T and 3.0 T MRI. Materials and Methods :
We reviewed 162 patients with primary lung cancer who were examined for TNM staging. After administration of double dose of Gd-DTPA, MR imaging was performed with SPGR by 3.0 T MRI and then with T1 SE sequence by 1.5 T MRI. In each patient, three readers performed qualitative assessment. Sensitivity, positive predictive value, and diagnostic accuracy were calculated in 3.0 T and 1.5 T MRI according to size. Using the signal intensity (SI) measurements between the metastatic nodules and adjacent tissue, nodule-to-adjacent tissue SI ratio was calculated. Results : Thirty-one of 162 patients had apparent metastatic nodules in the brain at either 1.5 T or 3.0 T MR imaging. 143 nodules were detected in 3.0 T MRI, whereas 137 nodules were detected at 1.5 T MRI. Six nodules, only detected in 3.0 T MRI, were smaller than 3.0 mm in dimension. Sensitivity, positive predictive value, and diagnostic accuracy in 3.0 T MRI were 100 %, 100 %, and 100 % respectively, and in 1.5 T MRI were 95.8 %, 88.3 %, and 85.1 % respectively. SI ratio was significantly higher in the 3.0 T MRI than 1.5 T MRI (p=0.025). Conclusion : True positive rate of 3.0 T MRI with Gd-DTPA was superior to 1.5 T MRI with Gd-DTPA in detection of metastatic nodules smaller than 3.0 mm. Index words :Magnetic resonance (MR), high-field-strength imaging Brain neoplasm, metastases Contrast medium Introduction Brain metastases present a poor prognosis suggesting a shortened survival time. Early diagnosis of brain involvement and determination of the number of metastases are important not only for quality of life but also for cost effectiveness (1-3).
The decision regarding a conservative versus a surgical approach depends on the number of brain metastases detected by radiologic means (1-3). A contrast-enhanced MRI has become the method of choice for visualization of brain metastases (1). High[1]dose gadolinium-enhanced MR examinations may have advantages over 0.1 mmol/kg examinations in detecting early and/or small metastases (3-7).
A delayed study can also increase the contrast (2). Comparing to the 1.5 T MRI with an axial T1-weighted spin echo sequence (SE), the higher field strength MR systems combined with a sequence of SPGR (spoiled gradient recalled acquisition in the steady state) and administration of a high dose of Gd-DTPA (gadopentetate dimeglumine) may also have advantages in detecting small metastases, although this has not yet been verified by clinical data. The purpose of this study is to compare the detectability of brain metastases classified according to the size of nodules, between thin slice SPGR of 3.0 T and conventional thick slice SE of 1.5 T MRI with the administration of a double dose of Gd[1]DTPA.
Materials and Methods Patients From December 2002 to February 2004, a total of 162 consecutive patients with primary lung cancer participated in our study.
The institutional review board approved our study, and informed consent was obtained from all patients regarding the potential risks of both the double dose of contrast medium and two assessments by MRI scanning on a 3.0 T and 1.5 T machine. After the study, 31 patients of this population were diagnosed as having brain metastases. Mean patient age was 61.2 (range, 43 to 80 years). Protocol On the 3.0 T MR scanner (GE Signa VH/i; GE medical system, Milwaukee, USA), the images were acquired using a standard head coil and an actively shielded gradient system with a maximum gradient strength of 43 mT/m. On the 1.5 T MR scanner (Magnetom Vision; Siemens Medical Systems, Erlangen, Germany), a standard head coil and a maximum gradient strength of 25 mT/m were used. All patients were examined after administrating a contrast agent with a double dose of Gd-DTPA (0.2 mmol/kg). First, examinations were performed on a 3.0 T MR scanner and then were subsequently performed on a 1.5 T MR scanner without additional contrast injection.
The scan interval between the 3.0 T and 1.5 T MR examination was less than 20 minutes. The contrast agent used was Gd-DTPA (Magnevist; Schering AG, Berlin, Germany). In all patients, the double dose of Gd-DTPA at 0.2 mmol/kg was administered intravenously as a bolus and scanning commenced immediately. MR imaging included the following sequences on both scanners:
At 3.0 T MRI, an axial 3D SPGR, which is usually used at present, was used (TR/TE/TI = 5.7/1.44/400 milliseconds; flip angle 20°; 2 mm slice thickness; FOV of 220 mm; matrix size of 512×512 ZIP; spatial resolution of 0.43×0.43×2 mm; two acquisition) with a scan time of 3 minutes 30 seconds. At 1.5 T MRI, an axial T1-weighted spin echo sequence was used (TR/RE = 600/14 milliseconds; flip angle 90°; 5 mm slice thickness; FOV of 210 mm; matrix size of 174×256; spatial resolution of 1.2×0.82×5 mm; two acquisition) with a scan time of 5 minutes 30 seconds.
Three radiologists performed randomized, independent blinded review. The three readers were merely informed that all of the patients had lung malignancies. The postcontrast MR examinations of the brain on all of the patients were evaluated. The readers did not have access to other image sets within each study. The presence, size, and number of metastatic nodules were assessed. The postcontrast images were divided into the following two groups: 3.0 T MRI with a double dose of Gd-DTPA and 1.5 T MRI with a double dose of Gd-DTPA. The readers were asked to document the number of nodules. Each nodule in each study was numbered and classified according to its largest diameter measurement: ≤3 mm, 3 mm to 5 mm, or >5 mm. Woo-Suk Chung et al – 102 – Subsequently, if there was any debate about nodule classification, a final interpretation using imaging studies was done until consensus among the readers was accomplished. If disagreements persisted, 3-6 months of follow-up MR scans were obtained for further validation.
For the patients who had follow-up MR scans, these scans were considered positive for metastases if there was a response to the treatment or if there was a growth of nodules identified during the follow-up period. In addition, the sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of the 3.0 T and 1.5 T MRI were calculated using the results from the final interpretation according to size. A quantitative image assessment was performed next. The same lesions on scans of the two different MRI systems were determined by comparing peripheral structures. Signal intensities of adjacent tissue and nodule were assessed by region of interest (ROI) measurements placed identically on both series of images using the same sized circular ROI from the software available on both scanners. Nodule-to[1]adjacent tissue contrast (SI ratio) is defined by SI ratio = ×100 Stissue1 taken as the signal intensity of an ROI assessed over a nodule and Stissue2 taken as the signal intensity assessed over the contralateral white matter.
The signal intensity of a nodule was measured within an enhanced area. In inhomogeneously enhanced nodules, the area of maximum uptake was chosen for measurement. Statistical Analysis The paired Wilcoxon’s signed ranks test was used to compare qualitative scores, and the matched-pair-t test was used to compare nodule SI ratios between the 3.0 T and 1.5 T MRI with a double dose of Gd-DTPA. For all tests, significance was set at p < 0.05, and SPSS software (SPSS Inc. Chicago, US) was used for statistical analyses. Results In the final review made by consensus of three radiologists (Table 1), a total of 143 metastatic nodules were detected by the 3.0 T MRI with a double dose of Gd-DTPA. Of these nodules, 49 nodules were ≤ 3 mm in diameter, 37 nodules were 3 mm to 5 mm, and 57 nodules were >5 mm. A total of 137 metastatic nodules were detected by the 1.5 T MRI with a double dose of Gd-DTPA in the final interpretation. Of these nodules, 43 nodules were ≤ 3 mm in diameter. The 3.0 T MRI with a double dose of Gd-DTPA was significantly more effective at detecting nodules smaller than 3 mm (p = 0.014) than the 1.5 T MRI. However, we found no significant difference in the detection of nodules larger than 3 mm (p > 0.05) (Table 1). In 6 of the 31 cases, six nodules, which were only detected by the 3.0 T MRI with a double dose of Gd[1]DTPA, and missed by the 1.5 T MRI with a double dose of Gd-DTPA, were unanimously agreed upon by all participants in the final interpretation. In three of the six nodules, a growing nodule was detected during a follow-up MR scan which confirmed the presence of metastases (Fig. 1). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of Gd-DTPA due to artifact (Fig. 2). Finally the 3.0 T MRI with a double dose of Gd-DTPA was Stissue1 – Stissue2 Stissue2 Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA – 103 – Table 1. Total Number of Brain Metastases Classified by Size and Detected at the Final Interpretation Size 3.0 T MRI with 1.5 T MRI with p value Gd-DTPA Gd-DPTA ≤ 3 mm 49 43 0.014 3 mm<-≤5 mm 37 37 > 0.05 5 mm< 57 57 > 0.05 Total 143 137 0.014 Note : Data are the number of nodules Table 2. The Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRIs with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm Present Absent Present Absent 3.0 T MRI with Positive 143 00* 49 0* Gd-DTPA Negatiive 000 00* 00 0* 1.5 T MRI with Positive 137 18* 43 18* Gd-DTPA Negative 006 00* 06 0* * Pseudolesions that were detected as nodules by the 1.5 T MRI were detected as vascular structures by the 3.0 T MRI. useful for confirming the presence of these nodules. Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter or better delineation than by the 1.5 T MRI with a double dose of Gd-DTPA. Out of 137 nodules, 65 were brighter (Fig. 3) and out of 137 nodules, 63 were better delineated (Fig. 4). Forty[1]five of 137 nodules were satisfactory in both conditions. By consensus, the final review stated, nodules detected by the 3.0 T and 1.5 T MRI were considered positive for metastases (Table 2). Additionally, there were 18 pseudolesions which were detected as nodules by the 1.5 T MRI, but as vascular structures by the 3.0 T MRI (Fig. 5). The sensitivity, positive predictive values, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 95.8%, 88.3%, and 85.1% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of the 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and Woo-Suk Chung et al – 104 – a b Fig. 2.
A 73-year-old male with multiple brain metastases. Metastatic nodule (a) by a 3.0 T MR image with a double dose of Gd-DTPA show a metastatic nodule (arrow). But (b) the 1.5 T MR image with a double dose of Gd-DTPA cannot show the metastatic nodule by artifact. abc Fig. 1. A 65-year-old male with single brain metastasis. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a small metastatic nodule (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA cannot show the nodule. In (c), a growing nodule was detected during the follow-up MRI with a double dose of Gd-DTPA which confirmed the presence of metastasis (arrow). 100% respectively. For metastatic nodules smaller than 3 mm, the sensitivity, positive predictive value, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 87.8%, 70.5%, and 64.2% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and 100% respectively (Table 3). For quantitative image assessment, the SI ratio in the post contrast sequences (Table 4) was significantly higher in the 3.0 T MRI with a double dose of Gd[1]DTPA than in the 1.5 T MRI with a double dose of Gd[1]DTPA (p = 0.025). Discussion Detection of metastatic nodules is dependent on both their size and contrast ratio (2). As methods to increase the contrast, a higher dose of Gd-DTPA, a higher field strength, and delayed study can all be used to aid detection (2-5, 8-17). Nodules larger than 10 mm are easily detected because vasogenic edema is customarily associated with larger metastases (2). So, when a higher dose of Gd-DTPA is used, the detection rate of larger nodules is not influenced. However, a higher dose is helpful for detecting small nodules because it increases nodule enhancement, yet this method has the disadvantages of increasing the false positive rate and promoting side effects (2-5, 8-14).
A delayed study can also increase the contrast (2). It has been recommended that image acquisition be delayed from 5 to 35 minutes after the administration of contrast material at a dose of 0.1 mmol/kg to ensure optimal detection (2, 15). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of Gd[1]DTPA due to partial volume artifact. Eighteen lesions were detected in the 1.5 T MRI with a double dose of Gd-DTPA, which proved to be vascular structures in 3.0 T MRI with a double dose of Gd- DTPA. The true nature of these lesions was revealed because of the greater morphologic detail visualized by the high field Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA – 105 – a b Fig. 3. A 65-year-old male with multiple brain metastases. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhancement (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhance[1]ment (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter than when observed by the 1.5 T MRI with a double dose of Gd[1]DTPA. Table 3. Estimation of the Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRI with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm 3.0 T 1.5T 3.0 T 1.5T Sensitivity 100 95.8 100 87.8 Specificity – 0 – 0 Positive predictive value 100 88.3 100 70.5 Negative predictive value – 0 – 0 Diagnostic accuracy 100 85.1 100 64.2 Table 4. Results of a quantitative assessment of nodules that were detected by the 3.0 T and 1.5 T MRIs with Gd-DTPA (n=137) 3.0 T 1.5 T P value Nodules-to-adjacent tissue: SI ratio 94.59 63.86 0.025 strength MR image, thus allowing differentiation between true enhancing lesions and sulcal vessels. In our study, each nodules was classified according to its largest diameter as being ≤ 3 mm, 3 mm to 5 mm, and >5 mm because the slice thickness of the 3.0 T MRI was 2.0 mm and 5 mm for the 1.5 T MRI. Therefore this study classified small metastatic nodules as being smaller than 3 mm. Although our study supports the use of a higher field strength MRI with a double dose of Gd-DTPA for increased metastatic nodule detection and for improved nodule enhancement and delineation, the results should be interpretated with caution.
The reason for this is that for patients with two or more brain metastases, additional metastases found with the 3.0 T MRI seem to be of limited clinical importance. The presence of two or more small nodules generally will not change the way the patient is managed. Therefore, it is of utmost importance to identify the difference between none, one, and more than one metastatic nodule.
Patients with a single metastatic nodule located in a respectable region can be treated surgically, and the tumor staged as M1, not M0. However, patients with two or more metastatic nodules are usually Woo-Suk Chung et al – 106 – a b Fig. 5. A 67-year-old female with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows vascular structure (arrow). (b) The 1.5 T MRI with a double dose of Gd[1]DTPA shows a nodular lesion (arrow). A pseudolesion that was detected as a nodule by the 1.5 T MRI with a double dose of Gd[1]DTPA but as a vascular structure by the 3.0 T MRI with a double dose of Gd-DTPA is showed in this figure. a b Fig. 4. A 64-year-old male with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows a metastatic nodule with ring enhancement (arrow). (b) The 1.5 T MRI with Gd-DTPA show a metastatic nodule with ring enhancement (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were better delineated than when observed by the 1.5 T MRI with a double dose of Gd[1]DTPA. treated with radiation therapy and/or systemic chemotherapy (3, 18-22). On the other hand, the use of a higher strength field MRI was found to be helpful in confirming the appearance of an equivocal metastatic nodule. The 3.0 T MRI with a double dose of Gd-DTPA was also useful for the detection of additional metastases in patients with a known lesion detected by the 1.5 T MRI with a double dose of Gd[1]DTPA. Because this also has influence on the sensitivity, positive predictive value, and diagnostic accuracy the 3.0 T MRI with a double dose of Gd[1]DTPA was found to have better results than the 1.5 T MRI with a double dose of Gd-DTPA in our study. Therefore we recommend the use of the 3.0 T MRI with a double dose of Gd-DTPA in only three circumstances: when the findings by the 1.5 T MRI with Gd-DTPA are equivocal, when one potentially surgically respectable nodule is identified, or for detecting early and/or small metastases
There were two limitations in this study. The first limitation was a difference in protocol sequence. The T1 weighted spin-echo protocol was used for the 1.5 T MRI and SPGR technique protocol for the 3.0 T MRI. Detectability of metastatic nodules is more effective with 3.0 T MRI with T1 SE than with a 1.5 T MRI with SE (2). SPGR with thin slice thickness is superior to the T1 spin echo sequence with thick slice thickness due to a partial volume effect. Additionally, SE is not optimum for a 3.0 T due to longer T1- and shorter T2- relaxation times of water protons, which decrease the contrast ratio in the 3.0 T images.17 The purpose of this study was to detect early small brain metastases, so using the SPGR sequence with a 3.0 T MRI, which is usually used at present, has advantages for detecting early small brain metastases. The second limitation was that the scan interval between the 1.5 T and 3.0 T MRI was less than 20 minutes. However, a delayed study increases contrast as mentioned above. The current study found that the SI ratio was significantly higher in the 3.0T images than in the 1.5 T images. Considering the delayed study by the 1.5 T MRI, this limitation emphasizes the better detection rate of the 3.0 T MRI with a double dose of Gd-DTPA. And due to these confounding variables, blinded reviews were performed by three readers. The detectability of metastatic nodules smaller than 3mm was better using a 3.0 T MRI with SPGR than a 1.5 T MRI with T1 SE. Therefore we recommend a 3.0 T MRI with SPGR and a double dose of Gd-DTPA for detecting early and/or small metastatic nodules, furthermore influencing treatment. References 1.Lassman AB, DeAngelis LM. Brain metastases. Neurol Clin. 2003; 21:1-23, vii, Review 2.Ba-Ssalamah A, Nobauer-Huhmann IM, Pinker K, et al. Effect of contrast dose and field strength in the magnetic resonance detection of brain metastases. Invest Radiol 2003; 38: 415-422 3.Sze G, Johnson C, Kawamura Y, et al. Comparison of single[1]and triple-dose contrast material in the MR screening of brain metastases. AJNR Am J Neuroradiol 1998; 19:821-828 4.Runge VM, Kirsch JE, Burke VJ, et al. High-dose Gadoteridol in MR imaging of intracranial neoplasm. J Magn Reson Imaging 1992; 2:9-18 5.Yuh WT, Engelken JD, Muhonen MG, Mayr NA, Fisher DJ, Ehrhardt JC. Experience with high-dose gadolinium MR imaging in the evaluation of brain metastases. AJNR Am J Neuroradiol 1992; 13:335-345 6.Brekenfeld C, Foert E, Hundt W, Kenn W, Lodeann KP, Gehl HB. Enhancement of cerebral diseases: How much contrast agent is enough? Comparison of 0.1, 0.2, and 0.3 mmol/kg Gadoteridol at 0.2 T with 0.1 mmol/kg Gadoteridol at 1.5 T. Invest Radiol 2001; 36:266-275 7.Yuh WT, Tali ET, Nguyen HD, Simonson TM, Mayr NA, Fisher DJ. The effect of contrast dose, imaging time, and lesion size in the MR detection of intracerebral metastasis. AJNR Am J Neuroradiol 1998; 16:373-380 8.Van Dijk P, Sijens PE, Schmitz PI, Oudkerk M. Gd-enhanced MR imaging of brain metastases: contrast as a function of dose and lesion size. Magn Reson Imaging 1997; 15:535-541 9.Yuh WT, Fisher DJ, Engelken JD, et al. MR evaluation of CNS tumors: dose comparison study with gadopentetate dimeglumine and gadoteridol. Radiology 1991; 180:485-491 10.Healy ME, Hasselink JR, Press GA, Middleton MS. Increased detection of intracranial metastases with intravenous Gd[1]DTPA. Radiology 1987; 165:619-624 11.Akeson P, Vikhoff B, Stahlberg F, Holtas S. Brain lesion contrast in MR imaging: dependence of field strength and concentration of gadodiamide injection in patients and phantoms. Acta Radiol 1977; 38:14-18 12.Runge VM. A review of contrast media research in 1999 – 2000. Invest Radiol 2001; 36:123-130 13.Yuh WT, Parker JR Carvlin MJ. Indication related dosing for magnetic resonance contrast media. Eur Radiol 1977; 7(suppl 5):S269-S275 14.Rinck PA, Muller RN. Field strength and dose dependence of contrast enhancement by Gadolinium-based MR contrast agents. Eur Radiol 1999; 9:998-1004 15.Schorner W, Laniado M, Niendorf HP, Schubert C, Felix R. Time-dependent changes in image contrast in brain tumors after gadolinium-DTPA. AJNR Am J Neuroradiol 1986; Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA – 107 – 7:1013-1020 16.Chang KH, Ra DG, Han MH, Cha SH, Kim HD, Han MC. Contrast enhancement of brain tumors at different MR field strengths: comparison of 0.5 T and 2.0 T. AJNR Am J Neuroradiol 1994; 15:1413-1419 17.Nobauer-Huhmann IM, Ba-Ssalamah A, Mlynarik V, et al. Magnetic resonance imaging contrast enhancement of brain tumors at 3 tesla versus 1.5 tesla. Invest Radiol 2002; 37:114- 119 18.Galicich JH, Sundaresan N, Thaler HT. Surgical treatment of single brain metastasis: evaluation of results by computerized tomography scanning. J Neurosurg 1980; 53:63-67 19.Runge VM, Carollo BR, Wolf CR, Nelson KL, Gelblum DY. Gd-DTPA: A review of clinical indications in central nervous system magnetic resonance imaging. Radiographics 1989; 9:929-958 20.Earnest F 4th, Ryu JH, Miller GM, et al. Suspected non-small cell lung cancer: Incidence of occult brain and skeletal metastases and effectiveness of imaging for detection-Pilot study. Radiology 1999; 211:137-145 21.Koutras AK, Marangos M, Kourelis T, et al. Surgical management of cerebral metastases from non-small cell lung cancer. Tumori 2003; 89:292-297 22.Soffietti R, Ruda R, Mutani R. Management of brain metastases. J Neurol 2002; 249:1357-1369. Review Woo-Suk Chung et al – 108 – 통신저자 : 정태섭, 서울특별시 강남구 도곡동 146-92 연세대학교 영동세브란스병원 영상의학과 Tel. 82-2019-3514 Fax. 82-3462-5472 E-mail: tschung@yumc.yonsei.ac.kr 뇌전이종양의발견에있어서Doble dose Gd-DTPA를이용한 3 T MRI와1.5 T MRI간의비교연구 1 연세대학교 영동세브란스병원 영상의학과 2 연세대학교 영동세브란스병원 호흡기내과 정우석1 ·정태섭1 ·김형중2 ·안철민2 ·이재훈1 ·허 진1 ·조응혁1 목적: 작은 뇌전이 종양의 조기 발견은 중요하다. 이 연구의 목적은 1.5 T MRI와 3.0 T MRI 간의 크기에 따른 뇌 전이 종양의 발견율을 비교하는 것이다. 대상 및 방법: 폐암으로 진단 받은 162명의 환자를 대상으로 TNM 병기를 위해 뇌 MRI를 시행하였다. Gd-DTPA 를 2배 용량으로 투여 후, 3.0 T MRI에서 훼손경사회복획득으로 촬영하였으며 그 후 1.5 T MRI에서 T1 스핀 에 코로 촬영하였다. 3명의 방사선과 전문의가 합의하여 MRI를 판독하였으며 정성 평가를 시행하였다. 3.0 T와 1.5 T MRI에서 크기에 따라 민감도, 양성 예측률, 정확도를 평가하였다. 신호 강도를 사용하여 전이 종양과 인접 조직간 의 신호강도 비를 계산하였다. 결과: 162명의 환자 중 31명에서 1.5 T 또는 3.0 T MR에 뇌전이 종양이 발견되었다. 3.0 T MRI에서 143개의 종 양이 발견되었으나 1.5 T MRI에서 137개의 종양이 발견되었다. 6개의 종양이 3.0 T MRI에서만 발견되었으며 크 기는 모두 3 mm 미만이었다. 3.0 T MRI의 민감도, 양성 예측률, 정확도는 각각 100%, 100%, 100%이며, 1.5 T MRI에서는 각각 95.8%, 88.3%, 85.1% 이다. SI ratio는 1.5 T MRI보다 3.0 T MRI에서 유의하게 높았다 (p=0.025). 결론: Double dose Gd-DTPA를 이용한 3.0 T MRI는 3 mm미만의 뇌전이 종양을 발견하는데 있어서 1.5 T
Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA Woo-Suk Chung, M.D.1 , Tae-Sub Chung, M.D.1 , Hyung Jung Kim, M.D.2 , Chul Min Ahn, M.D.2 , Jae Hoon Lee, M.D.1 , Jin Hur, M.D.1 , Arthur Eung-Hyuck Cho, M.D.1 Purpose : Early detection of small brain metastases is important. The purpose of this study was to compare the detectability of brain metastases according to the size between 1.5 T and 3.0 T MRI. Materials and Methods : We reviewed 162 patients with primary lung cancer who were examined for TNM staging. After administration of double dose of Gd-DTPA, MR imaging was performed with SPGR by 3.0 T MRI and then with T1 SE sequence by 1.5 T MRI. In each patient, three readers performed qualitative assessment. Sensitivity, positive predictive value, and diagnostic accuracy were calculated in 3.0 T and 1.5 T MRI according to size. Using the signal intensity (SI) measurements between the metastatic nodules and adjacent tissue, nodule-to-adjacent tissue SI ratio was calculated. Results : Thirty-one of 162 patients had apparent metastatic nodules in the brain at either 1.5 T or 3.0 T MR imaging. 143 nodules were detected in 3.0 T MRI, whereas 137 nodules were detected at 1.5 T MRI. Six nodules, only detected in 3.0 T MRI, were smaller than 3.0 mm in dimension. Sensitivity, positive predictive value, and diagnostic accuracy in 3.0 T MRI were 100 %, 100 %, and 100 % respectively, and in 1.5 T MRI were 95.8 %, 88.3 %, and 85.1 % respectively. SI ratio was significantly higher in the 3.0 T MRI than 1.5 T MRI (p=0.025). Conclusion : True positive rate of 3.0 T MRI with Gd-DTPA was superior to 1.5 T MRI with Gd-DTPA in detection of metastatic nodules smaller than 3.0 mm. Index words :Magnetic resonance (MR), high-field-strength imaging Brain neoplasm, metastases Contrast medium Introduction Brain metastases present a poor prognosis suggesting a shortened survival time. Early diagnosis of brain involvement and determination of the number of metastases are important not only for quality of life but also for cost effectiveness (1-3). The decision regarding a conservative versus a surgical approach depends on the number of brain metastases detected by radiologic means (1-3). A contrast-enhanced MRI has become the method of choice for visualization of brain metastases (1). Highdose gadolinium-enhanced MR examinations may have advantages over 0.1 mmol/kg examinations in detecting early and/or small metastases (3-7). A delayed study can also increase the contrast (2). Comparing to the 1.5 T MRI with an axial T1-weighted spin echo sequence (SE), the higher field strength MR systems combined with a sequence of SPGR (spoiled gradient recalled acquisition in the steady state) and administration of a high dose of Gd-DTPA (gadopentetate dimeglumine) may also have advantages in detecting small metastases, although this has not yet been verified by clinical data. The purpose of this study is to compare the detectability of brain metastases classified according to the size of nodules, between thin slice SPGR of 3.0 T and conventional thick slice SE of 1.5 T MRI with the administration of a double dose of GdDTPA. Materials and Methods Patients From December 2002 to February 2004, a total of 162 consecutive patients with primary lung cancer participated in our study. The institutional review board approved our study, and informed consent was obtained from all patients regarding the potential risks of both the double dose of contrast medium and two assessments by MRI scanning on a 3.0 T and 1.5 T machine. After the study, 31 patients of this population were diagnosed as having brain metastases. Mean patient age was 61.2 (range, 43 to 80 years). Protocol On the 3.0 T MR scanner (GE Signa VH/i; GE medical system, Milwaukee, USA), the images were acquired using a standard head coil and an actively shielded gradient system with a maximum gradient strength of 43 mT/m. On the 1.5 T MR scanner (Magnetom Vision; Siemens Medical Systems, Erlangen, Germany), a standard head coil and a maximum gradient strength of 25 mT/m were used. All patients were examined after administrating a contrast agent with a double dose of Gd-DTPA (0.2 mmol/kg). First, examinations were performed on a 3.0 T MR scanner and then were subsequently performed on a 1.5 T MR scanner without additional contrast injection. The scan interval between the 3.0 T and 1.5 T MR examination was less than 20 minutes. The contrast agent used was Gd-DTPA (Magnevist; Schering AG, Berlin, Germany). In all patients, the double dose of Gd-DTPA at 0.2 mmol/kg was administered intravenously as a bolus and scanning commenced immediately. MR imaging included the following sequences on both scanners: At 3.0 T MRI, an axial 3D SPGR, which is usually used at present, was used (TR/TE/TI = 5.7/1.44/400 milliseconds; flip angle 20°; 2 mm slice thickness; FOV of 220 mm; matrix size of 512×512 ZIP; spatial resolution of 0.43×0.43×2 mm; two acquisition) with a scan time of 3 minutes 30 seconds. At 1.5 T MRI, an axial T1-weighted spin echo sequence was used (TR/RE = 600/14 milliseconds; flip angle 90°; 5 mm slice thickness; FOV of 210 mm; matrix size of 174×256; spatial resolution of 1.2×0.82×5 mm; two acquisition) with a scan time of 5 minutes 30 seconds. Three radiologists performed randomized, independent blinded review. The three readers were merely informed that all of the patients had lung malignancies. The postcontrast MR examinations of the brain on all of the patients were evaluated. The readers did not have access to other image sets within each study. The presence, size, and number of metastatic nodules were assessed. The postcontrast images were divided into the following two groups: 3.0 T MRI with a double dose of Gd-DTPA and 1.5 T MRI with a double dose of Gd-DTPA. The readers were asked to document the number of nodules. Each nodule in each study was numbered and classified according to its largest diameter measurement: ≤3 mm, 3 mm to 5 mm, or
5 mm. Woo-Suk Chung et al
102 – Subsequently, if there was any debate about nodule classification, a final interpretation using imaging studies was done until consensus among the readers was accomplished. If disagreements persisted, 3-6 months of follow-up MR scans were obtained for further validation. For the patients who had follow-up MR scans, these scans were considered positive for metastases if there was a response to the treatment or if there was a growth of nodules identified during the follow-up period. In addition, the sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of the 3.0 T and 1.5 T MRI were calculated using the results from the final interpretation according to size. A quantitative image assessment was performed next. The same lesions on scans of the two different MRI systems were determined by comparing peripheral structures. Signal intensities of adjacent tissue and nodule were assessed by region of interest (ROI) measurements placed identically on both series of images using the same sized circular ROI from the software available on both scanners. Nodule-toadjacent tissue contrast (SI ratio) is defined by SI ratio = ×100 Stissue1 taken as the signal intensity of an ROI assessed over a nodule and Stissue2 taken as the signal intensity assessed over the contralateral white matter. The signal intensity of a nodule was measured within an enhanced area. In inhomogeneously enhanced nodules, the area of maximum uptake was chosen for measurement. Statistical Analysis The paired Wilcoxon’s signed ranks test was used to compare qualitative scores, and the matched-pair-t test was used to compare nodule SI ratios between the 3.0 T and 1.5 T MRI with a double dose of Gd-DTPA. For all tests, significance was set at p < 0.05, and SPSS software (SPSS Inc. Chicago, US) was used for statistical analyses. Results In the final review made by consensus of three radiologists (Table 1), a total of 143 metastatic nodules were detected by the 3.0 T MRI with a double dose of Gd-DTPA. Of these nodules, 49 nodules were ≤ 3 mm in diameter, 37 nodules were 3 mm to 5 mm, and 57 nodules were >5 mm. A total of 137 metastatic nodules were detected by the 1.5 T MRI with a double dose of Gd-DTPA in the final interpretation. Of these nodules, 43 nodules were ≤ 3 mm in diameter. The 3.0 T MRI with a double dose of Gd-DTPA was significantly more effective at detecting nodules smaller than 3 mm (p = 0.014) than the 1.5 T MRI. However, we found no significant difference in the detection of nodules larger than 3 mm (p > 0.05) (Table 1). In 6 of the 31 cases, six nodules, which were only detected by the 3.0 T MRI with a double dose of GdDTPA, and missed by the 1.5 T MRI with a double dose of Gd-DTPA, were unanimously agreed upon by all participants in the final interpretation. In three of the six nodules, a growing nodule was detected during a follow-up MR scan which confirmed the presence of metastases (Fig. 1). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of Gd-DTPA due to artifact (Fig. 2). Finally the 3.0 T MRI with a double dose of Gd-DTPA was Stissue1 – Stissue2 Stissue2 Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA
103 – Table 1. Total Number of Brain Metastases Classified by Size and Detected at the Final Interpretation Size 3.0 T MRI with 1.5 T MRI with p value Gd-DTPA Gd-DPTA ≤ 3 mm 49 43 0.014 3 mm<-≤5 mm 37 37 > 0.05 5 mm< 57 57 > 0.05 Total 143 137 0.014 Note : Data are the number of nodules Table 2. The Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRIs with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm Present Absent Present Absent 3.0 T MRI with Positive 143 00* 49 0* Gd-DTPA Negatiive 000 00* 00 0* 1.5 T MRI with Positive 137 18* 43 18* Gd-DTPA Negative 006 00* 06 0*
Pseudolesions that were detected as nodules by the 1.5 T MRI were detected as vascular structures by the 3.0 T MRI. useful for confirming the presence of these nodules. Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter or better delineation than by the 1.5 T MRI with a double dose of Gd-DTPA. Out of 137 nodules, 65 were brighter (Fig. 3) and out of 137 nodules, 63 were better delineated (Fig. 4). Fortyfive of 137 nodules were satisfactory in both conditions. By consensus, the final review stated, nodules detected by the 3.0 T and 1.5 T MRI were considered positive for metastases (Table 2). Additionally, there were 18 pseudolesions which were detected as nodules by the 1.5 T MRI, but as vascular structures by the 3.0 T MRI (Fig. 5). The sensitivity, positive predictive values, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 95.8%, 88.3%, and 85.1% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of the 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and Woo-Suk Chung et al
104 – a b Fig. 2. A 73-year-old male with multiple brain metastases. Metastatic nodule (a) by a 3.0 T MR image with a double dose of Gd-DTPA show a metastatic nodule (arrow). But (b) the 1.5 T MR image with a double dose of Gd-DTPA cannot show the metastatic nodule by artifact. abc Fig. 1. A 65-year-old male with single brain metastasis. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a small metastatic nodule (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA cannot show the nodule. In (c), a growing nodule was detected during the follow-up MRI with a double dose of Gd-DTPA which confirmed the presence of metastasis (arrow). 100% respectively. For metastatic nodules smaller than 3 mm, the sensitivity, positive predictive value, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 87.8%, 70.5%, and 64.2% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and 100% respectively (Table 3). For quantitative image assessment, the SI ratio in the post contrast sequences (Table 4) was significantly higher in the 3.0 T MRI with a double dose of GdDTPA than in the 1.5 T MRI with a double dose of GdDTPA (p = 0.025). Discussion Detection of metastatic nodules is dependent on both their size and contrast ratio (2). As methods to increase the contrast, a higher dose of Gd-DTPA, a higher field strength, and delayed study can all be used to aid detection (2-5, 8-17). Nodules larger than 10 mm are easily detected because vasogenic edema is customarily associated with larger metastases (2). So, when a higher dose of Gd-DTPA is used, the detection rate of larger nodules is not influenced. However, a higher dose is helpful for detecting small nodules because it increases nodule enhancement, yet this method has the disadvantages of increasing the false positive rate and promoting side effects (2-5, 8-14). A delayed study can also increase the contrast (2). It has been recommended that image acquisition be delayed from 5 to 35 minutes after the administration of contrast material at a dose of 0.1 mmol/kg to ensure optimal detection (2, 15). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of GdDTPA due to partial volume artifact. Eighteen lesions were detected in the 1.5 T MRI with a double dose of Gd-DTPA, which proved to be vascular structures in 3.0 T MRI with a double dose of Gd- DTPA. The true nature of these lesions was revealed because of the greater morphologic detail visualized by the high field Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA
105 – a b Fig. 3. A 65-year-old male with multiple brain metastases. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhancement (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhancement (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter than when observed by the 1.5 T MRI with a double dose of GdDTPA. Table 3. Estimation of the Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRI with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm 3.0 T 1.5T 3.0 T 1.5T Sensitivity 100 95.8 100 87.8 Specificity – 0 – 0 Positive predictive value 100 88.3 100 70.5 Negative predictive value – 0 – 0 Diagnostic accuracy 100 85.1 100 64.2 Table 4. Results of a quantitative assessment of nodules that were detected by the 3.0 T and 1.5 T MRIs with Gd-DTPA (n=137) 3.0 T 1.5 T P value Nodules-to-adjacent tissue: SI ratio 94.59 63.86 0.025 strength MR image, thus allowing differentiation between true enhancing lesions and sulcal vessels. In our study, each nodules was classified according to its largest diameter as being ≤ 3 mm, 3 mm to 5 mm, and >5 mm because the slice thickness of the 3.0 T MRI was 2.0 mm and 5 mm for the 1.5 T MRI. Therefore this study classified small metastatic nodules as being smaller than 3 mm. Although our study supports the use of a higher field strength MRI with a double dose of Gd-DTPA for increased metastatic nodule detection and for improved nodule enhancement and delineation, the results should be interpretated with caution. The reason for this is that for patients with two or more brain metastases, additional metastases found with the 3.0 T MRI seem to be of limited clinical importance. The presence of two or more small nodules generally will not change the way the patient is managed. Therefore, it is of utmost importance to identify the difference between none, one, and more than one metastatic nodule. Patients with a single metastatic nodule located in a respectable region can be treated surgically, and the tumor staged as M1, not M0. However, patients with two or more metastatic nodules are usually Woo-Suk Chung et al
106 – a b Fig. 5. A 67-year-old female with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows vascular structure (arrow). (b) The 1.5 T MRI with a double dose of GdDTPA shows a nodular lesion (arrow). A pseudolesion that was detected as a nodule by the 1.5 T MRI with a double dose of GdDTPA but as a vascular structure by the 3.0 T MRI with a double dose of Gd-DTPA is showed in this figure. a b Fig. 4. A 64-year-old male with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows a metastatic nodule with ring enhancement (arrow). (b) The 1.5 T MRI with Gd-DTPA show a metastatic nodule with ring enhancement (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were better delineated than when observed by the 1.5 T MRI with a double dose of GdDTPA. treated with radiation therapy and/or systemic chemotherapy (3, 18-22). On the other hand, the use of a higher strength field MRI was found to be helpful in confirming the appearance of an equivocal metastatic nodule. The 3.0 T MRI with a double dose of Gd-DTPA was also useful for the detection of additional metastases in patients with a known lesion detected by the 1.5 T MRI with a double dose of GdDTPA. Because this also has influence on the sensitivity, positive predictive value, and diagnostic accuracy the 3.0 T MRI with a double dose of GdDTPA was found to have better results than the 1.5 T MRI with a double dose of Gd-DTPA in our study. Therefore we recommend the use of the 3.0 T MRI with a double dose of Gd-DTPA in only three circumstances: when the findings by the 1.5 T MRI with Gd-DTPA are equivocal, when one potentially surgically respectable nodule is identified, or for detecting early and/or small metastases There were two limitations in this study. The first limitation was a difference in protocol sequence. The T1 weighted spin-echo protocol was used for the 1.5 T MRI and SPGR technique protocol for the 3.0 T MRI. Detectability of metastatic nodules is more effective with 3.0 T MRI with T1 SE than with a 1.5 T MRI with SE (2). SPGR with thin slice thickness is superior to the T1 spin echo sequence with thick slice thickness due to a partial volume effect. Additionally, SE is not optimum for a 3.0 T due to longer T1- and shorter T2- relaxation times of water protons, which decrease the contrast ratio in the 3.0 T images.17 The purpose of this study was to detect early small brain metastases, so using the SPGR sequence with a 3.0 T MRI, which is usually used at present, has advantages for detecting early small brain metastases. The second limitation was that the scan interval between the 1.5 T and 3.0 T MRI was less than 20 minutes. However, a delayed study increases contrast as mentioned above. The current study found that the SI ratio was significantly higher in the 3.0T images than in the 1.5 T images. Considering the delayed study by the 1.5 T MRI, this limitation emphasizes the better detection rate of the 3.0 T MRI with a double dose of Gd-DTPA. And due to these confounding variables, blinded reviews were performed by three readers. The detectability of metastatic nodules smaller than 3mm was better using a 3.0 T MRI with SPGR than a 1.5 T MRI with T1 SE. Therefore we recommend a 3.0 T MRI with SPGR and a double dose of Gd-DTPA for detecting early and/or small metastatic nodules, furthermore influencing treatment. References 1.Lassman AB, DeAngelis LM. Brain metastases. Neurol Clin. 2003; 21:1-23, vii, Review 2.Ba-Ssalamah A, Nobauer-Huhmann IM, Pinker K, et al. Effect of contrast dose and field strength in the magnetic resonance detection of brain metastases. Invest Radiol 2003; 38: 415-422 3.Sze G, Johnson C, Kawamura Y, et al. Comparison of singleand triple-dose contrast material in the MR screening of brain metastases. AJNR Am J Neuroradiol 1998; 19:821-828 4.Runge VM, Kirsch JE, Burke VJ, et al. High-dose Gadoteridol in MR imaging of intracranial neoplasm. J Magn Reson Imaging 1992; 2:9-18 5.Yuh WT, Engelken JD, Muhonen MG, Mayr NA, Fisher DJ, Ehrhardt JC. Experience with high-dose gadolinium MR imaging in the evaluation of brain metastases. AJNR Am J Neuroradiol 1992; 13:335-345 6.Brekenfeld C, Foert E, Hundt W, Kenn W, Lodeann KP, Gehl HB. Enhancement of cerebral diseases: How much contrast agent is enough? Comparison of 0.1, 0.2, and 0.3 mmol/kg Gadoteridol at 0.2 T with 0.1 mmol/kg Gadoteridol at 1.5 T. Invest Radiol 2001; 36:266-275 7.Yuh WT, Tali ET, Nguyen HD, Simonson TM, Mayr NA, Fisher DJ. The effect of contrast dose, imaging time, and lesion size in the MR detection of intracerebral metastasis. AJNR Am J Neuroradiol 1998; 16:373-380 8.Van Dijk P, Sijens PE, Schmitz PI, Oudkerk M. Gd-enhanced MR imaging of brain metastases: contrast as a function of dose and lesion size. Magn Reson Imaging 1997; 15:535-541 9.Yuh WT, Fisher DJ, Engelken JD, et al. MR evaluation of CNS tumors: dose comparison study with gadopentetate dimeglumine and gadoteridol. Radiology 1991; 180:485-491 10.Healy ME, Hasselink JR, Press GA, Middleton MS. Increased detection of intracranial metastases with intravenous GdDTPA. Radiology 1987; 165:619-624 11.Akeson P, Vikhoff B, Stahlberg F, Holtas S. Brain lesion contrast in MR imaging: dependence of field strength and concentration of gadodiamide injection in patients and phantoms. Acta Radiol 1977; 38:14-18 12.Runge VM. A review of contrast media research in 1999 –
Invest Radiol 2001; 36:123-130 13.Yuh WT, Parker JR Carvlin MJ. Indication related dosing for magnetic resonance contrast media. Eur Radiol 1977; 7(suppl 5):S269-S275 14.Rinck PA, Muller RN. Field strength and dose dependence of contrast enhancement by Gadolinium-based MR contrast agents. Eur Radiol 1999; 9:998-1004 15.Schorner W, Laniado M, Niendorf HP, Schubert C, Felix R. Time-dependent changes in image contrast in brain tumors after gadolinium-DTPA. AJNR Am J Neuroradiol 1986; Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA
107 – 7:1013-1020 16.Chang KH, Ra DG, Han MH, Cha SH, Kim HD, Han MC. Contrast enhancement of brain tumors at different MR field strengths: comparison of 0.5 T and 2.0 T. AJNR Am J Neuroradiol 1994; 15:1413-1419 17.Nobauer-Huhmann IM, Ba-Ssalamah A, Mlynarik V, et al. Magnetic resonance imaging contrast enhancement of brain tumors at 3 tesla versus 1.5 tesla. Invest Radiol 2002; 37:114- 119 18.Galicich JH, Sundaresan N, Thaler HT. Surgical treatment of single brain metastasis: evaluation of results by computerized tomography scanning. J Neurosurg 1980; 53:63-67 19.Runge VM, Carollo BR, Wolf CR, Nelson KL, Gelblum DY. Gd-DTPA: A review of clinical indications in central nervous system magnetic resonance imaging. Radiographics 1989; 9:929-958 20.Earnest F 4th, Ryu JH, Miller GM, et al. Suspected non-small cell lung cancer: Incidence of occult brain and skeletal metastases and effectiveness of imaging for detection-Pilot study. Radiology 1999; 211:137-145 21.Koutras AK, Marangos M, Kourelis T, et al. Surgical management of cerebral metastases from non-small cell lung cancer. Tumori 2003; 89:292-297 22.Soffietti R, Ruda R, Mutani R. Management of brain metastases. J Neurol 2002; 249:1357-1369. Review
Neuro Second Opinion Catches Missed Brain Lesions Suggestive of MS
4/16/20
Malcolm’s brain MRI was initially read as completely normal. Upon getting a second opinion, it was discovered that 22 lesions suggestive of multiple sclerosis had been missed. Here is his story.
[Malcolm] After 18 months of deteriorating health, with a multitude of neurological symptoms, I went to see a neurologist. I was ordered a standard brain MRI to help figure out what was going on. By this time, I had been researching my symptoms for a few months, and, in doing so, had developed a basic understanding of what I was looking for: T2 lesions.
When I received the results from my MRI, the report said everything was normal. I met with my neurologist, and he too said there was nothing abnormal about my scan. When I viewed the MRI myself, however, I found 4 spots that looked to me to be brain lesions. I brought them up to my doctor at my next appointment but was essentially laughed at.
It was quite unsettling to have something so concerning be shrugged off. After that appointment, I decided I wanted to switch to a new neurologist and get a second opinion on my MRI scan. I made an appointment with the new doctor, but it was going to be another 6 weeks before I could be seen. Fortunately, I found DocPanel. I submitted my MRI for review and, within 48 hours, I got my results back.
[Dr. Michael Rozenfeld] Malcolm reached out to DocPanel due to concern for a missed diagnosis. He was reportedly having symptoms suspicious for multiple sclerosis but his MRI was initially read as completely normal. Based on my review of his MRI, the exam was not normal. Malcolm had significant findings that were certainly suggestive of, but not entirely specific for, multiple sclerosis.
[Malcolm] My second opinion results were quite alarming – there were not 4 lesions, but 22. Twenty-two! They were small, but they were most definitely there. I took the second opinion report to my new neurologist, and now I am being considered for possible Primary Progressive Multiple Sclerosis. I am scheduled to get new MRIs in November to confirm or rule out MS and you can be sure I will be sending them to DocPanel for a second look!
I have found that the most important thing people in my shoes can do is be your own advocate. MS is such an odd and individual disease. – Malcolm
[Dr. Michael Rozenfeld] Radiology exams can be misinterpreted for a number of reasons – this is unfortunately not uncommon. While MRI is not the only piece in the puzzle for MS diagnosis, it plays a significant role. A false negative diagnosis made off an MRI scan could lead the neurologist and patient down an incorrect path and delay an accurate diagnosis, or potentially miss it entirely.
While MRI is not the only piece in the puzzle for MS diagnosis, it plays a significant role. A false negative diagnosis made off an MRI scan could lead the neurologist and patient down an incorrect path and delay an accurate diagnosis, or potentially miss it entirely.
The positive findings on Malcolm’s exam and his new report provide additional essential information for his neurologist, allowing him (the neurologist) to combine these imaging findings with other test results and physical exam findings to come to an accurate diagnosis.
I would always suggest patients seek a second opinion for complex medical diagnoses, especially if the patient feels that something is being missed or that their concerns aren’t being addressed. This could mean setting up an appointment with a second neurologist or submitting your radiology exams for a second opinion to a company such as DocPanel, where they will be interpreted by subspecialty trained and certified neuroradiologists. I personally like to explain the imaging findings in layman’s terms, to ensure that the patient understands the disease process. I believe this empowers patients so that they can take an active role in ensuring the best decisions regarding their care are made.
[Malcolm] After a few months of working with my current neurologist and a support group of people diagnosed with MS, I have found that the most important thing people in my shoes can do is be your own advocate. MS is such an odd, and individual disease. No two patients are exactly alike in their presentation or their symptoms. This can make it very difficult to diagnose. It is always helpful to get several opinions; your health is just to darn important.
DocPanel is committed to making sure every patient receives excellent care. If you would like an expert second opinion on your medical imaging scan from Dr.Rozenfeld or one of our other neuroradiology subspecialists, you can learn morehere.
Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA Woo-Suk Chung, M.D.1 , Tae-Sub Chung, M.D.1 , Hyung Jung Kim, M.D.2 , Chul Min Ahn, M.D.2 , Jae Hoon Lee, M.D.1 , Jin Hur, M.D.1 , Arthur Eung-Hyuck Cho, M.D.1 Purpose : Early detection of small brain metastases is important.
The purpose of this study was to compare the detectability of brain metastases according to the size between 1.5 T and 3.0 T MRI. Materials and Methods :
We reviewed 162 patients with primary lung cancer who were examined for TNM staging. After administration of double dose of Gd-DTPA, MR imaging was performed with SPGR by 3.0 T MRI and then with T1 SE sequence by 1.5 T MRI. In each patient, three readers performed qualitative assessment. Sensitivity, positive predictive value, and diagnostic accuracy were calculated in 3.0 T and 1.5 T MRI according to size. Using the signal intensity (SI) measurements between the metastatic nodules and adjacent tissue, nodule-to-adjacent tissue SI ratio was calculated. Results : Thirty-one of 162 patients had apparent metastatic nodules in the brain at either 1.5 T or 3.0 T MR imaging. 143 nodules were detected in 3.0 T MRI, whereas 137 nodules were detected at 1.5 T MRI. Six nodules, only detected in 3.0 T MRI, were smaller than 3.0 mm in dimension. Sensitivity, positive predictive value, and diagnostic accuracy in 3.0 T MRI were 100 %, 100 %, and 100 % respectively, and in 1.5 T MRI were 95.8 %, 88.3 %, and 85.1 % respectively. SI ratio was significantly higher in the 3.0 T MRI than 1.5 T MRI (p=0.025). Conclusion : True positive rate of 3.0 T MRI with Gd-DTPA was superior to 1.5 T MRI with Gd-DTPA in detection of metastatic nodules smaller than 3.0 mm. Index words :Magnetic resonance (MR), high-field-strength imaging Brain neoplasm, metastases Contrast medium Introduction Brain metastases present a poor prognosis suggesting a shortened survival time. Early diagnosis of brain involvement and determination of the number of metastases are important not only for quality of life but also for cost effectiveness (1-3).
The decision regarding a conservative versus a surgical approach depends on the number of brain metastases detected by radiologic means (1-3). A contrast-enhanced MRI has become the method of choice for visualization of brain metastases (1). High[1]dose gadolinium-enhanced MR examinations may have advantages over 0.1 mmol/kg examinations in detecting early and/or small metastases (3-7).
A delayed study can also increase the contrast (2). Comparing to the 1.5 T MRI with an axial T1-weighted spin echo sequence (SE), the higher field strength MR systems combined with a sequence of SPGR (spoiled gradient recalled acquisition in the steady state) and administration of a high dose of Gd-DTPA (gadopentetate dimeglumine) may also have advantages in detecting small metastases, although this has not yet been verified by clinical data. The purpose of this study is to compare the detectability of brain metastases classified according to the size of nodules, between thin slice SPGR of 3.0 T and conventional thick slice SE of 1.5 T MRI with the administration of a double dose of Gd[1]DTPA.
Materials and Methods Patients From December 2002 to February 2004, a total of 162 consecutive patients with primary lung cancer participated in our study.
The institutional review board approved our study, and informed consent was obtained from all patients regarding the potential risks of both the double dose of contrast medium and two assessments by MRI scanning on a 3.0 T and 1.5 T machine. After the study, 31 patients of this population were diagnosed as having brain metastases. Mean patient age was 61.2 (range, 43 to 80 years). Protocol On the 3.0 T MR scanner (GE Signa VH/i; GE medical system, Milwaukee, USA), the images were acquired using a standard head coil and an actively shielded gradient system with a maximum gradient strength of 43 mT/m. On the 1.5 T MR scanner (Magnetom Vision; Siemens Medical Systems, Erlangen, Germany), a standard head coil and a maximum gradient strength of 25 mT/m were used. All patients were examined after administrating a contrast agent with a double dose of Gd-DTPA (0.2 mmol/kg). First, examinations were performed on a 3.0 T MR scanner and then were subsequently performed on a 1.5 T MR scanner without additional contrast injection.
The scan interval between the 3.0 T and 1.5 T MR examination was less than 20 minutes. The contrast agent used was Gd-DTPA (Magnevist; Schering AG, Berlin, Germany). In all patients, the double dose of Gd-DTPA at 0.2 mmol/kg was administered intravenously as a bolus and scanning commenced immediately. MR imaging included the following sequences on both scanners:
At 3.0 T MRI, an axial 3D SPGR, which is usually used at present, was used (TR/TE/TI = 5.7/1.44/400 milliseconds; flip angle 20°; 2 mm slice thickness; FOV of 220 mm; matrix size of 512×512 ZIP; spatial resolution of 0.43×0.43×2 mm; two acquisition) with a scan time of 3 minutes 30 seconds. At 1.5 T MRI, an axial T1-weighted spin echo sequence was used (TR/RE = 600/14 milliseconds; flip angle 90°; 5 mm slice thickness; FOV of 210 mm; matrix size of 174×256; spatial resolution of 1.2×0.82×5 mm; two acquisition) with a scan time of 5 minutes 30 seconds.
Three radiologists performed randomized, independent blinded review. The three readers were merely informed that all of the patients had lung malignancies. The postcontrast MR examinations of the brain on all of the patients were evaluated. The readers did not have access to other image sets within each study. The presence, size, and number of metastatic nodules were assessed. The postcontrast images were divided into the following two groups: 3.0 T MRI with a double dose of Gd-DTPA and 1.5 T MRI with a double dose of Gd-DTPA. The readers were asked to document the number of nodules. Each nodule in each study was numbered and classified according to its largest diameter measurement: ≤3 mm, 3 mm to 5 mm, or >5 mm. Woo-Suk Chung et al – 102 – Subsequently, if there was any debate about nodule classification, a final interpretation using imaging studies was done until consensus among the readers was accomplished. If disagreements persisted, 3-6 months of follow-up MR scans were obtained for further validation.
For the patients who had follow-up MR scans, these scans were considered positive for metastases if there was a response to the treatment or if there was a growth of nodules identified during the follow-up period. In addition, the sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of the 3.0 T and 1.5 T MRI were calculated using the results from the final interpretation according to size. A quantitative image assessment was performed next. The same lesions on scans of the two different MRI systems were determined by comparing peripheral structures. Signal intensities of adjacent tissue and nodule were assessed by region of interest (ROI) measurements placed identically on both series of images using the same sized circular ROI from the software available on both scanners. Nodule-to[1]adjacent tissue contrast (SI ratio) is defined by SI ratio = ×100 Stissue1 taken as the signal intensity of an ROI assessed over a nodule and Stissue2 taken as the signal intensity assessed over the contralateral white matter.
The signal intensity of a nodule was measured within an enhanced area. In inhomogeneously enhanced nodules, the area of maximum uptake was chosen for measurement. Statistical Analysis The paired Wilcoxon’s signed ranks test was used to compare qualitative scores, and the matched-pair-t test was used to compare nodule SI ratios between the 3.0 T and 1.5 T MRI with a double dose of Gd-DTPA. For all tests, significance was set at p < 0.05, and SPSS software (SPSS Inc. Chicago, US) was used for statistical analyses. Results In the final review made by consensus of three radiologists (Table 1), a total of 143 metastatic nodules were detected by the 3.0 T MRI with a double dose of Gd-DTPA. Of these nodules, 49 nodules were ≤ 3 mm in diameter, 37 nodules were 3 mm to 5 mm, and 57 nodules were >5 mm. A total of 137 metastatic nodules were detected by the 1.5 T MRI with a double dose of Gd-DTPA in the final interpretation. Of these nodules, 43 nodules were ≤ 3 mm in diameter. The 3.0 T MRI with a double dose of Gd-DTPA was significantly more effective at detecting nodules smaller than 3 mm (p = 0.014) than the 1.5 T MRI. However, we found no significant difference in the detection of nodules larger than 3 mm (p > 0.05) (Table 1). In 6 of the 31 cases, six nodules, which were only detected by the 3.0 T MRI with a double dose of Gd[1]DTPA, and missed by the 1.5 T MRI with a double dose of Gd-DTPA, were unanimously agreed upon by all participants in the final interpretation. In three of the six nodules, a growing nodule was detected during a follow-up MR scan which confirmed the presence of metastases (Fig. 1). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of Gd-DTPA due to artifact (Fig. 2). Finally the 3.0 T MRI with a double dose of Gd-DTPA was Stissue1 – Stissue2 Stissue2 Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA – 103 – Table 1. Total Number of Brain Metastases Classified by Size and Detected at the Final Interpretation Size 3.0 T MRI with 1.5 T MRI with p value Gd-DTPA Gd-DPTA ≤ 3 mm 49 43 0.014 3 mm<-≤5 mm 37 37 > 0.05 5 mm< 57 57 > 0.05 Total 143 137 0.014 Note : Data are the number of nodules Table 2. The Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRIs with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm Present Absent Present Absent 3.0 T MRI with Positive 143 00* 49 0* Gd-DTPA Negatiive 000 00* 00 0* 1.5 T MRI with Positive 137 18* 43 18* Gd-DTPA Negative 006 00* 06 0* * Pseudolesions that were detected as nodules by the 1.5 T MRI were detected as vascular structures by the 3.0 T MRI. useful for confirming the presence of these nodules. Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter or better delineation than by the 1.5 T MRI with a double dose of Gd-DTPA. Out of 137 nodules, 65 were brighter (Fig. 3) and out of 137 nodules, 63 were better delineated (Fig. 4). Forty[1]five of 137 nodules were satisfactory in both conditions. By consensus, the final review stated, nodules detected by the 3.0 T and 1.5 T MRI were considered positive for metastases (Table 2). Additionally, there were 18 pseudolesions which were detected as nodules by the 1.5 T MRI, but as vascular structures by the 3.0 T MRI (Fig. 5). The sensitivity, positive predictive values, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 95.8%, 88.3%, and 85.1% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of the 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and Woo-Suk Chung et al – 104 – a b Fig. 2.
A 73-year-old male with multiple brain metastases. Metastatic nodule (a) by a 3.0 T MR image with a double dose of Gd-DTPA show a metastatic nodule (arrow). But (b) the 1.5 T MR image with a double dose of Gd-DTPA cannot show the metastatic nodule by artifact. abc Fig. 1. A 65-year-old male with single brain metastasis. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a small metastatic nodule (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA cannot show the nodule. In (c), a growing nodule was detected during the follow-up MRI with a double dose of Gd-DTPA which confirmed the presence of metastasis (arrow). 100% respectively. For metastatic nodules smaller than 3 mm, the sensitivity, positive predictive value, and diagnostic accuracy of the 1.5 T MRI with a double dose of Gd-DTPA were 87.8%, 70.5%, and 64.2% respectively. The sensitivity, positive predictive value, and diagnostic accuracy of 3.0 T MRI with a double dose of Gd-DTPA were 100%, 100%, and 100% respectively (Table 3). For quantitative image assessment, the SI ratio in the post contrast sequences (Table 4) was significantly higher in the 3.0 T MRI with a double dose of Gd[1]DTPA than in the 1.5 T MRI with a double dose of Gd[1]DTPA (p = 0.025). Discussion Detection of metastatic nodules is dependent on both their size and contrast ratio (2). As methods to increase the contrast, a higher dose of Gd-DTPA, a higher field strength, and delayed study can all be used to aid detection (2-5, 8-17). Nodules larger than 10 mm are easily detected because vasogenic edema is customarily associated with larger metastases (2). So, when a higher dose of Gd-DTPA is used, the detection rate of larger nodules is not influenced. However, a higher dose is helpful for detecting small nodules because it increases nodule enhancement, yet this method has the disadvantages of increasing the false positive rate and promoting side effects (2-5, 8-14).
A delayed study can also increase the contrast (2). It has been recommended that image acquisition be delayed from 5 to 35 minutes after the administration of contrast material at a dose of 0.1 mmol/kg to ensure optimal detection (2, 15). Three of the 6 nodules missed were unable to be detected using the 1.5 T MRI with a double dose of Gd[1]DTPA due to partial volume artifact. Eighteen lesions were detected in the 1.5 T MRI with a double dose of Gd-DTPA, which proved to be vascular structures in 3.0 T MRI with a double dose of Gd- DTPA. The true nature of these lesions was revealed because of the greater morphologic detail visualized by the high field Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA – 105 – a b Fig. 3. A 65-year-old male with multiple brain metastases. (a) The 3.0 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhancement (arrow). (b) The 1.5 T MR image with a double dose of Gd-DTPA shows a metastatic nodule with spherical enhance[1]ment (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were brighter than when observed by the 1.5 T MRI with a double dose of Gd[1]DTPA. Table 3. Estimation of the Values of Currently Used Statistical Measures for the 3.0 T and 1.5 T MRI with Gd-DTPA According to Nodule Size Metastatic nodules Total ≤ 3 mm 3.0 T 1.5T 3.0 T 1.5T Sensitivity 100 95.8 100 87.8 Specificity – 0 – 0 Positive predictive value 100 88.3 100 70.5 Negative predictive value – 0 – 0 Diagnostic accuracy 100 85.1 100 64.2 Table 4. Results of a quantitative assessment of nodules that were detected by the 3.0 T and 1.5 T MRIs with Gd-DTPA (n=137) 3.0 T 1.5 T P value Nodules-to-adjacent tissue: SI ratio 94.59 63.86 0.025 strength MR image, thus allowing differentiation between true enhancing lesions and sulcal vessels. In our study, each nodules was classified according to its largest diameter as being ≤ 3 mm, 3 mm to 5 mm, and >5 mm because the slice thickness of the 3.0 T MRI was 2.0 mm and 5 mm for the 1.5 T MRI. Therefore this study classified small metastatic nodules as being smaller than 3 mm. Although our study supports the use of a higher field strength MRI with a double dose of Gd-DTPA for increased metastatic nodule detection and for improved nodule enhancement and delineation, the results should be interpretated with caution.
The reason for this is that for patients with two or more brain metastases, additional metastases found with the 3.0 T MRI seem to be of limited clinical importance. The presence of two or more small nodules generally will not change the way the patient is managed. Therefore, it is of utmost importance to identify the difference between none, one, and more than one metastatic nodule.
Patients with a single metastatic nodule located in a respectable region can be treated surgically, and the tumor staged as M1, not M0. However, patients with two or more metastatic nodules are usually Woo-Suk Chung et al – 106 – a b Fig. 5. A 67-year-old female with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows vascular structure (arrow). (b) The 1.5 T MRI with a double dose of Gd[1]DTPA shows a nodular lesion (arrow). A pseudolesion that was detected as a nodule by the 1.5 T MRI with a double dose of Gd[1]DTPA but as a vascular structure by the 3.0 T MRI with a double dose of Gd-DTPA is showed in this figure. a b Fig. 4. A 64-year-old male with multiple brain metastases. (a) The 3.0 T MRI with a double dose of Gd-DTPA shows a metastatic nodule with ring enhancement (arrow). (b) The 1.5 T MRI with Gd-DTPA show a metastatic nodule with ring enhancement (arrow). Nodules observed by the 3.0 T MRI with a double dose of Gd-DTPA were better delineated than when observed by the 1.5 T MRI with a double dose of Gd[1]DTPA. treated with radiation therapy and/or systemic chemotherapy (3, 18-22). On the other hand, the use of a higher strength field MRI was found to be helpful in confirming the appearance of an equivocal metastatic nodule. The 3.0 T MRI with a double dose of Gd-DTPA was also useful for the detection of additional metastases in patients with a known lesion detected by the 1.5 T MRI with a double dose of Gd[1]DTPA. Because this also has influence on the sensitivity, positive predictive value, and diagnostic accuracy the 3.0 T MRI with a double dose of Gd[1]DTPA was found to have better results than the 1.5 T MRI with a double dose of Gd-DTPA in our study. Therefore we recommend the use of the 3.0 T MRI with a double dose of Gd-DTPA in only three circumstances: when the findings by the 1.5 T MRI with Gd-DTPA are equivocal, when one potentially surgically respectable nodule is identified, or for detecting early and/or small metastases
There were two limitations in this study. The first limitation was a difference in protocol sequence. The T1 weighted spin-echo protocol was used for the 1.5 T MRI and SPGR technique protocol for the 3.0 T MRI. Detectability of metastatic nodules is more effective with 3.0 T MRI with T1 SE than with a 1.5 T MRI with SE (2). SPGR with thin slice thickness is superior to the T1 spin echo sequence with thick slice thickness due to a partial volume effect. Additionally, SE is not optimum for a 3.0 T due to longer T1- and shorter T2- relaxation times of water protons, which decrease the contrast ratio in the 3.0 T images.17 The purpose of this study was to detect early small brain metastases, so using the SPGR sequence with a 3.0 T MRI, which is usually used at present, has advantages for detecting early small brain metastases. The second limitation was that the scan interval between the 1.5 T and 3.0 T MRI was less than 20 minutes. However, a delayed study increases contrast as mentioned above. The current study found that the SI ratio was significantly higher in the 3.0T images than in the 1.5 T images. Considering the delayed study by the 1.5 T MRI, this limitation emphasizes the better detection rate of the 3.0 T MRI with a double dose of Gd-DTPA. And due to these confounding variables, blinded reviews were performed by three readers. The detectability of metastatic nodules smaller than 3mm was better using a 3.0 T MRI with SPGR than a 1.5 T MRI with T1 SE. Therefore we recommend a 3.0 T MRI with SPGR and a double dose of Gd-DTPA for detecting early and/or small metastatic nodules, furthermore influencing treatment. References 1.Lassman AB, DeAngelis LM. Brain metastases. Neurol Clin. 2003; 21:1-23, vii, Review 2.Ba-Ssalamah A, Nobauer-Huhmann IM, Pinker K, et al. Effect of contrast dose and field strength in the magnetic resonance detection of brain metastases. Invest Radiol 2003; 38: 415-422 3.Sze G, Johnson C, Kawamura Y, et al. Comparison of single[1]and triple-dose contrast material in the MR screening of brain metastases. AJNR Am J Neuroradiol 1998; 19:821-828 4.Runge VM, Kirsch JE, Burke VJ, et al. High-dose Gadoteridol in MR imaging of intracranial neoplasm. J Magn Reson Imaging 1992; 2:9-18 5.Yuh WT, Engelken JD, Muhonen MG, Mayr NA, Fisher DJ, Ehrhardt JC. Experience with high-dose gadolinium MR imaging in the evaluation of brain metastases. AJNR Am J Neuroradiol 1992; 13:335-345 6.Brekenfeld C, Foert E, Hundt W, Kenn W, Lodeann KP, Gehl HB. Enhancement of cerebral diseases: How much contrast agent is enough? Comparison of 0.1, 0.2, and 0.3 mmol/kg Gadoteridol at 0.2 T with 0.1 mmol/kg Gadoteridol at 1.5 T. Invest Radiol 2001; 36:266-275 7.Yuh WT, Tali ET, Nguyen HD, Simonson TM, Mayr NA, Fisher DJ. The effect of contrast dose, imaging time, and lesion size in the MR detection of intracerebral metastasis. AJNR Am J Neuroradiol 1998; 16:373-380 8.Van Dijk P, Sijens PE, Schmitz PI, Oudkerk M. Gd-enhanced MR imaging of brain metastases: contrast as a function of dose and lesion size. Magn Reson Imaging 1997; 15:535-541 9.Yuh WT, Fisher DJ, Engelken JD, et al. MR evaluation of CNS tumors: dose comparison study with gadopentetate dimeglumine and gadoteridol. Radiology 1991; 180:485-491 10.Healy ME, Hasselink JR, Press GA, Middleton MS. Increased detection of intracranial metastases with intravenous Gd[1]DTPA. Radiology 1987; 165:619-624 11.Akeson P, Vikhoff B, Stahlberg F, Holtas S. Brain lesion contrast in MR imaging: dependence of field strength and concentration of gadodiamide injection in patients and phantoms. Acta Radiol 1977; 38:14-18 12.Runge VM. A review of contrast media research in 1999 – 2000. Invest Radiol 2001; 36:123-130 13.Yuh WT, Parker JR Carvlin MJ. Indication related dosing for magnetic resonance contrast media. Eur Radiol 1977; 7(suppl 5):S269-S275 14.Rinck PA, Muller RN. Field strength and dose dependence of contrast enhancement by Gadolinium-based MR contrast agents. Eur Radiol 1999; 9:998-1004 15.Schorner W, Laniado M, Niendorf HP, Schubert C, Felix R. Time-dependent changes in image contrast in brain tumors after gadolinium-DTPA. AJNR Am J Neuroradiol 1986; Evaluation between 3.0 T vs 1.5 T MRI in Detection of Brain Metastasis using Double Dose Gd-DTPA – 107 – 7:1013-1020 16.Chang KH, Ra DG, Han MH, Cha SH, Kim HD, Han MC. Contrast enhancement of brain tumors at different MR field strengths: comparison of 0.5 T and 2.0 T. AJNR Am J Neuroradiol 1994; 15:1413-1419 17.Nobauer-Huhmann IM, Ba-Ssalamah A, Mlynarik V, et al. Magnetic resonance imaging contrast enhancement of brain tumors at 3 tesla versus 1.5 tesla. Invest Radiol 2002; 37:114- 119 18.Galicich JH, Sundaresan N, Thaler HT. Surgical treatment of single brain metastasis: evaluation of results by computerized tomography scanning. J Neurosurg 1980; 53:63-67 19.Runge VM, Carollo BR, Wolf CR, Nelson KL, Gelblum DY. Gd-DTPA: A review of clinical indications in central nervous system magnetic resonance imaging. Radiographics 1989; 9:929-958 20.Earnest F 4th, Ryu JH, Miller GM, et al. Suspected non-small cell lung cancer: Incidence of occult brain and skeletal metastases and effectiveness of imaging for detection-Pilot study. Radiology 1999; 211:137-145 21.Koutras AK, Marangos M, Kourelis T, et al. Surgical management of cerebral metastases from non-small cell lung cancer. Tumori 2003; 89:292-297 22.Soffietti R, Ruda R, Mutani R. Management of brain metastases. J Neurol 2002; 249:1357-1369. Review Woo-Suk Chung et al – 108 – 통신저자 : 정태섭, 서울특별시 강남구 도곡동 146-92 연세대학교 영동세브란스병원 영상의학과 Tel. 82-2019-3514 Fax. 82-3462-5472 E-mail: tschung@yumc.yonsei.ac.kr 뇌전이종양의발견에있어서Doble dose Gd-DTPA를이용한 3 T MRI와1.5 T MRI간의비교연구 1 연세대학교 영동세브란스병원 영상의학과 2 연세대학교 영동세브란스병원 호흡기내과 정우석1 ·정태섭1 ·김형중2 ·안철민2 ·이재훈1 ·허 진1 ·조응혁1 목적: 작은 뇌전이 종양의 조기 발견은 중요하다. 이 연구의 목적은 1.5 T MRI와 3.0 T MRI 간의 크기에 따른 뇌 전이 종양의 발견율을 비교하는 것이다. 대상 및 방법: 폐암으로 진단 받은 162명의 환자를 대상으로 TNM 병기를 위해 뇌 MRI를 시행하였다. Gd-DTPA 를 2배 용량으로 투여 후, 3.0 T MRI에서 훼손경사회복획득으로 촬영하였으며 그 후 1.5 T MRI에서 T1 스핀 에 코로 촬영하였다. 3명의 방사선과 전문의가 합의하여 MRI를 판독하였으며 정성 평가를 시행하였다. 3.0 T와 1.5 T MRI에서 크기에 따라 민감도, 양성 예측률, 정확도를 평가하였다. 신호 강도를 사용하여 전이 종양과 인접 조직간 의 신호강도 비를 계산하였다. 결과: 162명의 환자 중 31명에서 1.5 T 또는 3.0 T MR에 뇌전이 종양이 발견되었다. 3.0 T MRI에서 143개의 종 양이 발견되었으나 1.5 T MRI에서 137개의 종양이 발견되었다. 6개의 종양이 3.0 T MRI에서만 발견되었으며 크 기는 모두 3 mm 미만이었다. 3.0 T MRI의 민감도, 양성 예측률, 정확도는 각각 100%, 100%, 100%이며, 1.5 T MRI에서는 각각 95.8%, 88.3%, 85.1% 이다. SI ratio는 1.5 T MRI보다 3.0 T MRI에서 유의하게 높았다 (p=0.025). 결론: Double dose Gd-DTPA를 이용한 3.0 T MRI는 3 mm미만의 뇌전이 종양을 발견하는데 있어서 1.5 T
Not everyone has access to a computer or internet but I am totally inspired by my contact who is 91 having to stand up for her son who by the sounds of it has been totally misdiagnosed and denied the correct pathological tests by the NHS.
A Carer’s Story by “A” (I am using the exact words of my guest blogger as written in a letter by request)
“I have been involved with Mental health for many years as a carer for my son, even though the diagnosis is totally wrong.
My son has had nothing but persecution – stress – no life whatsoever.
Resistant to some medications.
The service should provide the resistance test, only then would patients be on the right medication.
It would save a lot of problems – also a lot of money.
Most of all – The misery that these medications cause. They are addictive and very difficult to withdraw from.
It needs a special clinic, experienced person to make sure the withdrawal is successful.
My son has two disabilities from the medication.
He is in a wheelchair for over 20 years suffering from TD – Tardive Dyskinesia from the medication – injury to the brain – spine (Clozapine) no dopamin in this system
Disability (Risperidone) – brain disturbance so now lacks capacity.
They only knew one thing – pills/Tablets.
The system needs to change. Put the right people in the right jobs.
Mental health destroys everything ? (The system).”
I can only hope 2024 will be better than the last.
Xmas was the worst I have known for a long time. Elizabeth was not allowed home and wanted to see her cat but this was not allowed not even for one day. She is still held under heavy restrictions by Lincolnshire Partnership Trust on a never-ending section with phone taken away. The phone restriction has been going on for some time along with visiting restrictions said to be an MDT decision but we know that this is not the case. Restrictions commenced every two weeks, then a further two weeks and then increased to every four weeks up until 26 January. Even more restrictions seem now to be in place because when I have phoned following New Year since I had not spoken to Elizabeth for some time, several staff appeared reluctant to even hand the phone to her. The Clinical Lead, ES, stated the phone would only be given if Elizabeth specifically asked for it, others said “I will see if she wants to speak to you”. I know for a fact rest of family not treated the same but taking the phone away is very nasty and very restrictive and this is NHS not private sector care. Taking the phone away and locking it in the office or wherever makes it difficult for everyone in the family to keep in touch with Elizabeth who is cut off from the outside world and held a virtual prisoner after 2.5 years. It is not easy to get through to the ward. This is cruelty and I see it as punishment no doubt aimed at me but inflicting upon Elizabeth. Also, Elizabeth is deprived of playing her music on her phone and seeing pictures of her cat who she misses so much. She no longer has a life and neither do I, our lives ruined by the decision I made to move to what we thought was a lovely area. I have made a huge mistake moving here as although the immediate area is lovely I had not bargained for how ruthless the NHS is under MH care or the fact provision in the community is poor. Having said that, there is so much going on in the local area, things that Elizabeth would enjoy but instead she is locked up by a group of strangers(MDT) who think they know best and could not care less about the impact their punishment is having on the family, even those who are not under restriction are affected by taking the phone away yet there is no consideration whatsoever towards anyone. It is also forgotten about values, medical ethics and duty of care according to their individual Code of Conduct. They are in fact acting ultra vires by depriving s17 ground leave to the shop as a means of punishment for instance as instructed.
Xmas Eve, rest of family visited and reported Elizabeth “not so good”.
Xmas Day could not relax, cook a nice dinner or have people over this year. I had just 45 minutes with a member of staff supervising in the small visitor’s room. Elizabeth was OK at first but when the second member of staff took over she became upset by this person then a group gathered outside the visitor’s room and I was told to leave. I had heard through Elizabeth that she had a reduction in her medication and I wanted to know what reduction she had and it was very upsetting that so many staff outside grabbed hold of her and that is when she tried to defend herself but so many of them involved and all she did was shout at them. Police were called to the ward yet again by staff told to report concerns yet these concerns were nothing like I was accused of. It is alarming how many times Police have been called, as if they do not have enough to do for no reason. Always there has been nothing to report and no evidence whatsoever recorded on CCTV, only members of staff who are told to report adversely so as to make me out to be someone who is hostile, aggressive, etc. I now do not ever visit alone as I feel I am up against so many who are against me. So Xmas was awful. I had no idea Police had been called after I had left the premises that day. The first I knew about this was on the 28th December at on line ward round. I was told I was banned indefinitely by the RC for inciting Elizabeth to attack staff which was totally untrue. I have since received another unsigned letter from the MHA legal office stating the ban is four weeks until 26 January. They are not following NHS Guidelines and have no regard to the latest Government paper on hospital/care home visits or Code of Conduct of the MHA. It seems like a never-ending ban just like Elizabeth’s never-ending section – an imprisonment for life by LPFT. I have just been told I must no longer contact the carers champion. I must only write to one designated email address. Since moving, I have had no carer’s assessment and was actually told previously I was not entitled to this.
Most disturbingly of all, the Neurologist appointment on the 3 January was not attended by Elizabeth and when I questioned why, I was told by ES, Clinical Lead that nothing was in the diary and no one knew anything about it. Again this is totally untrue. It is obvious LPFT did not want her to either have an MRI scan all along or see a Neurologist or Endocrinologist in the first instance. It seems the most important thing is the drugs they force and the law they twist to suit themselves re MHA and MCA. All her physical health appointments were cancelled as unnecessary upon our move. I am also banned from taking Elizabeth to any physical health appointments. Our treatment has been even more appalling than the former area and I thought that was bad.
There does not seem to be any regard for human rights or Codes of Conduct/Guidelines.
For anyone else going through hell as we are I am going to share with you some points of law as what I am seeing is a whole group of professionals sticking together, totally disregarding their own code of conduct and ignoring the law. There seems to be no accountability. Some of these professionals are responsible for health and wellfare of the most vulnerable patients but what has happened is several have acted ultra vires relying on colleagues and MDT backing, going along with what they are instructed to do regardless of what is correct and according to law and medical ethics and they are in breach of their own code of conduct. Already restrictively detained under s3 MHA , Elizabeth is excessively deprived of any kind of liberty whatsoever, treated like a object not a person. It should be the least restrictive care under MHA but under LPFT, detention is more like what you would expect a restricted prisoner to have and no one seems to care less or to give a thought as to how they would feel if they were treated in this most degrading and undignified manner as Elizabeth is:
“It is no longer adequate for a medical practitioner to invoke the opinions of colleagues as authority for a decision. That mechanism known from the case of Bolam v. Friern Hospital Committee [1957] WLR 582
There is very strict policy as regards takeaways and Elizabeth loves Saturdays on the ward when patients are allowed to order a takeaway. Whilst I would agree that takeaways are not good on a daily basis, there have been occasions where Elizabeth has been so tired she has missed all her meals and been in bed most of the day. This is because of the huge amount of drugs prescribed have taken away every bit of quality of life leaving her with no energy and nothing but tiredness. I have drawn to attention of staff that missing meals is very bad and can affect behaviour but any sign of hostility is met with punishment and deprival of ground leave like one nurse did. Even though she was instructed, she still went along with it and this is surely not part of her role to dish out punishment, therefore she is acting ultra vires. On another occasion when without warning I was banned we thought we were going to the Carlton Shopping Centre but this was cancelled on the spur of the moment without warning by the RC of Castle Ward and Elizabeth was visibly upset. I had promised a meal for her and brought food to the ward and was told by a nurse that it was not permitted and to take that away along with gifts a friend brought. It was totally undignified as Elizabeth was looking through a slit in the glass door and could see we had arrived and we were told to leave the premises and that it was an Executive decision. I was told to get away from the door by another nurse as it was upsetting to Elizabeth. Again acting upon orders by banning a visitor to see a vulnerable patient who was excited and expecting our visit in her non existent life and these nurses stood in the way in the course of doing their job yet they acted ultra vires. It is not part of their job to ban visitors and then say it is an MDT or an Executive Decision not theirs when in fact they are the ones acting against their own Code of Conduct and even Trust Policy states about dignified care. Their actions along with the other nurse was totally undignified and degrading.
DENYING FOOD PARCELS AND TO ORDER FOOD FROM OUTSIDE
L v Board of State Hospital [2011] CSOH 21; 2011 SLT 233
The hospital had been ultra vires in denying patients the right to have food parcels and to order food from outside.
Whilst I agree ordering of takeaways every single day is not good or healthy but neither is missing meal times and there should always be exceptions but such is the environment, more restrictive than any prison this verges on abuse.
House of Commons House of Lords
Joint Committee on Human Rights
Protecting human rights in care settings
Fourth Report of Session 2022–23
Report, together with formal minutes relating to the report
Ordered by the House of Commons to be printed 13 July 2022
Ordered by the House of Lords to be printed 13 July 2022
HC 216 HL Paper 51
Published on 22 July 2022
by authority of the House of Commons and the House of Lords
This is a very interesting paper to read.
Joint Committee on Human Rights
The Joint Committee on Human Rights is appointed by the House of Lords and the House of Commons to consider matters relating to human rights in the United Kingdom (but excluding consideration of individual cases); proposals for remedial orders, draft remedial orders and remedial orders.
The Joint Committee has a maximum of six Members appointed by each House, of whom the quorum for any formal proceedings is two from each House.
Current membership
House of Commons
Harriet Harman QC MP (Labour, Camberwell and Peckham) (Chair)
Joanna Cherry QC MP (Scottish National Party, Edinburgh South West)
Florence Eshalomi MP (Labour, Vauxhall)
Angela Richardson MP (Conservative, Guildford)
Dean Russell MP (Conservative, Watford)
David Simmonds MP (Conservative, Ruislip, Northwood and Pinner)
House of Lords
Baroness Chisholm of Owlpen (Conservative)
Lord Dubs (Labour)
Lord Henley (Conservative)
Baroness Ludford (Liberal Democrat)
Baroness Massey of Darwen (Labour)
Lord Singh of Wimbledon (Crossbench)
“We were also concerned to hear about ongoing issues with Deprivation of Liberty Safeguards (DoLS), the check that is put in place to ensure that detention in care settings is within the law and in line with the prohibition of torture and inhuman or degrading treatment under Article 3 ECHR, and the right to liberty and security, under Article 5 ECHR. There are often unacceptable delays in authorisation of DoLS and there is often no access to legal aid if care users wish to challenge their deprivation of liberty in court. Whilst the DoLS system is going to be replaced by a new Liberty Protection Safeguards System (LPS), there is no timetable for this to be rolled out. We ask that the Government must work with the regulator and all stakeholders to ensure that providers fully understand the functioning DoLS and comply with statutory requirements, and that access to legal aid for those who wish to challenge is widened. The Government should also set a timetable for rollout of the LPS system and keep us updated on progress.
We have reported before on the visiting arrangements for those in care settings during the pandemic. Evidence submitted to this inquiry showed that through and beyond the pandemic problems persisted with providers following guidance. We also believe a lesson learnt from the pandemic was the harm caused by blanket bans on visiting. We have called in the past for the Government to legislate and do so again here. The Government must introduce legislation to secure to care users the right to nominate one or more individuals to visit and to provide support or care in all circumstances, subject to the same infection prevention and control rules as care staff. The Government must also legislate to give the CQC the power to require care settings to inform them of any changes to their visiting status, and to report live data on levels of visiting and restrictions. The CQC must make compliance with visiting restrictions a key consideration when undertaking its regulatory and monitoring roles.
Under the HRA, public authorities must act compatibly with ECHR rights. Those providing care services in care settings, however, are not all public authorities. Unless care legislation, such as the Care Act 2014, contract law, or consumer standards provide equivalent protections, there is no way for privately funded individuals in private care settings to enforce human rights on the same basis as for those in publicly funded care settings. This can mean that two residents in the same care home might have different legally enforceable rights. We recommend that the Government should consult on extending the protections of the HRA to those receiving care and support from all regulated providers, and suggest a way this could be done through an amendment of the Care Act 2014.
When something goes wrong, the users of a service should have access to an effective complaints mechanism that is capable of investigating those complaints, and putting things right, in a way that is transparent, fair, and proportionate. However, the complaints system for care users is confusing, time consuming and too often does not result in effective resolution. The system needs to become easier to navigate. Care users must not be frightened of retribution if they complain. We recommend changes to streamline the process, with the roles of the CQC, the Local Government and Social Care Ombudsman (LGSCO), and the Parliamentary and Health Service Ombudsman (PHSO) clarified and with all three organisations operating a “no wrong door policy”.
The right to life (Article 2 ECHR, Article 10 CRPD).
• Freedom from torture and inhuman or degrading treatment or punishment (Article 3 ECHR; Article 15 CRPD).
• The right to liberty and security (Article 5 ECHR; Article 14 CRPD).
• The right to family and private life (Article 8 ECHR; Articles 22 and 23 CRPD).
• Freedom from discrimination in the enjoyment of human rights (Article 14 ECHR; Article 5 CRPD).
• The right to the highest attainable standard of health (Article 12 International Covenant on Economic, Social and Cultural Rights (ICESCR); Article 25 CRPD).
ARTICLE 3 DEGRADING TREATMENT WHICH APPLIES TO ELIZABETH WHO IS HAVING FORCED INJECTIONS VIRTUALLY ON A DAILY BASIS.
ARTICLE 3 HRA
The failure to give her appropriate treatment for a condition she has been diagnosed as having creates a situation where she is subjected to inhumane and degrading treatment. Elizabeth has complex PTSD which is totally ignored by LPFT along with her physical health.
Constant Restraint and frequent RT is in breach of Art 3.
Deprivation of family rights is a consequence of this. They say she is dangerous but have done nothing to address that, apart from to subject her to close surveillance at all times. Elizabeth likes animals and adores her cat and pigeons. She is totally misunderstood by these professionals and I would say her treatment at times has been that of cruelty and abuse.
This is in violation of her rights under Art.3 ECHR and represents inhumane and degrading treatment as in Sławomir Musiał v.Poland (2009) & Raffray Taddei v. France (2010)
Incidentally the ECHR has ruled that whatever obstacles the patient may have put in front of the treatment team that did not dispense the state from its obligations to protect their human right to being protected from inhumane and degrading treatment, Claes v. Belgium (2013).
Right to take legal proceedings, ECHR Article 5(4) Storck v. Germany (Application No 61603/00), 16 June 2005.
Article 5(3), which deals with the rights of a person who has been detained.
“Everyone arrested or detained in accordance with the provisions of paragraph 1(c) of this article shall be brought promptly before a judge or other officer authorised by law to exercise judicial power and shall be entitled to trial within a reasonable time or to release pending trial. . . .”
The difference between a right to “take proceedings” and a right to “be brought promptly before a [court]” must be deliberate. It stops short of requiring judicial authorisation in every case.
It leaves to the person detained the choice of whether or not to put the matter before a court. MH (by her litigation friend, Official Solicitor) (FC) (Respondent) v. Secretary of State for the Department of Health (Appellant) and others.
Code of Conduct from the Nursing Midwifery Council and would comment on one or two points here:
1 Treat people as individuals and uphold their dignity To achieve this, you must:
1.1 treat people with kindness, respect and compassion
1.5 respect and uphold people’s human rights
3.4 act as an advocate for the vulnerable, challenging poor practice and discriminatory attitudes and behaviour relating to their care
4.4 tell colleagues, your manager and the person receiving care if you have a conscientious objection to a particular procedure and arrange for a suitably qualified colleague to take over responsibility for that person’s care
iv) A person is not to be treated as unable to make a decision merely because he or she makes a decision that is unwise (see Heart of England NHS Foundation Trust v JB [2014] EWHC 342 (COP)at [7]). The outcome of the decision made is not relevant to the question of whether the person taking the decision has capacity for the purposes of the Mental Capacity Act 2005 (see R v Cooper [2009] 1 WLR 1786at [13] and York City Council v C [2014] 2 WLR 1 at [53] and [54]);[2]
Masterman-Lister v Brutton & Co 2003
The leading case is Masterman-Lister v Brutton& Co [2003] 3 All ER 162 in which Lord Justice Chadwick stated at paragraph 75: the test to be applied….is whether the party to legal proceedings is capable of understanding, with the assistance of such proper explanation from legal advisors and experts in other disciplines as the case may require, the issues on which his consent or decision is likely to be necessary in the course of those proceedings. If he has capacity to understand that which he needs to understand in order to pursue or defend a claim, I can see no reason why the law – whether substantive or procedural – should require the imposition of … a litigation friend and at paragraph 79: a person should not be held unable to understand the information relevant to a decision if he can understand an explanation of that information in broad terms and simple language; and … he should not be regarded as unable to make a rational decision merely because the decision which he does in fact make is a decision which would not be made by a person of ordinary prudence. The Court of Appeal re-considered the Masterman-Lister test in Bailey v Warren [2006] EWCA Civ 51. At paragraph 126 of her judgment Lady Justice Arden concluded: The assessment of capacity to conduct proceedings depends to some extent on the nature of the proceedings in contemplation. I can only indicate some of the matters to be considered in accessing a client’s capacity. The client would need to understand how the proceedings were to be funded. He would need to know about the chances of not succeeding and about the risk of an adverse order as to costs. He would need to have capacity to make the sort of decisions that arise in litigation. Capacity to conduct such proceedings would include the capacity to give proper instructions for and to approve the particulars of claim, and to approve a compromise. For a client to have capacity to approve a compromise, he would need insight into the compromise, an ability to instruct his solicitors to advise him on it, and an understanding of their advice and an ability to weigh their advice Capacity to conduct proceedings was further considered by the Supreme Court in the post-MCA case of Dunhill v Burgin (Nos 1 and 2) [2014] UKSC 18. At paragraph 13 of her judgment Lady Hale noted: The general approach of the common law, now confirmed in the Mental Capacity Act 2005, is that capacity is to be judged in relation to the decision or activity in question and not globally. Hence it was concluded in Masterman-Lister that capacity for this purpose meant capacity to conduct the proceedings (which might be different from capacity to administer a large award resulting from the proceedings). This was also the test adopted by the majority of the Court of Appeal in Bailey v Warren[2006] EWCA Civ 51, [2006] CP Rep 26, where Arden LJ specifically related it to the capacity to commence the proceedings (para 112). It would have been open to the parties in this court to challenge
that test, based as it was mainly upon first instance decisions in relation to litigation and the general principle that capacity is issue specific, but neither has done so. In my view, the Court of Appeal reached the correct conclusion on this point in Masterman-Lister and there is no need for us to repeat the reasoning which is fully set out in the judgment of Chadwick LJ.
Subject:Guidelines on Restricting Hospital Visits
Visits from friends and relatives are considered crucial in the recovery and welfare of patients and research carried out on the severe restrictions imposed during the Covid pandemic indicates a clear detrimental effect on patients who missed visits from loved ones and friends. The impact on visitors has also resulted in an increased incidence of depression and anxiety being recorded. Elizabeth had once enjoyed my visits and especially on just one occasion the two hour leave unescorted at the Carlton Centre just around the corner from the hospital.
Excluding or restricting visits should therefore be imposed only in exceptional circumstances where there are reasonable ground for believing that a visitor may have a detrimental effect on the patients therapy. I have been told I am indefinitely banned by the RC but in order to do that surely an application should have been made by LPFT to the Court of Protection to get rid of me for good. What they are doing is very wrong.
A decision to exclude visitors on the grounds of his or her behaviour or propensities must be fully documented and explained to the patient and where possible the appropriate person concerned. In the case of psychiatric patients the nearest relative should be informed of any visitor exclusions and supervision decision and if it is they who are excluded or supervised an explanation in writing is to be provided to them. Nothing has been done properly. The nearest relative who I became nearest relative to has most certainly not been informed and no proper explanation has been given other than I am said by the RC to be a “bad influence”. I am even said to be partly the cause of the episodes that look like fits but most of these have taken place when I have not been around. The real reason is that they want to send her far away from home and family and cut contact altogether and they are doing this by isolating Elizabeth from her family already.
A visitor may be excluded or restricted to visits under supervision if the visit is considered to be anti-therapeutic (in the short or long term) to an extent that a discernible arrest of progress or even deterioration of the patient’s mental state is evident or can reasonably be anticipated if contact is not restricted. It is the MDT of so many, none of whom take individual responsibility who do not want me to visit and why? It has been said “why do you think Everyone ….…….. everyone agrees with his decision, everyone of practically 30 who are invited to MDT meetings agree and every one of them going along with EXECUTIVE decision made by one or two who do not want me on the premises because they do not want information shared. That is the real reason.
An impact assessment should be carried out in consultation with the patient to assess the impact of any denial or restriction of visits on the patient’s welfare. Where a patient lacks capacity or is impaired as to their capacity an assessment by a suitably qualified best interests assessor should be carried out to assess any negative impact that denial or restriction of visits may have on the patient.
Here is the impact these professionals are having on my daughter as stated on Xmas Day “I no longer wish to live”. This is the effect of the so called “care” by LPFT rated good by the CQC. It is the worse experience we have ever encountered.
CLINICAL CARE LPFT TRUST POLICY DOCUMENT
8. Admission to Hospital/Keeping an individual in hospital
8.1 Policy Statement Care in a residential or hospital setting should be provided at the lowest level of security and restriction based on an individualised assessment of need, risk and capacity. Alternatives to residential or hospital care such as home treatment and crisis intervention should be considered as a less restrictive alternative to hospital admission where possible.
8.2 Consent to Admission to Hospital/Keeping Someone in Hospital If the individual has the capacity to decide whether to come into hospital or remain in hospital, then informed consent should be sought in all cases. This means that the individual is given information about the environment, routine and purpose of the inpatient setting / admission. If the individual does not consent, then consideration should be given to assessment and admission under the Mental Health Act (MHA) see MHA Policy 6a. If the individual does not have capacity to consent to hospital admission, then the MHA should be considered or the Mental Capacity Act (MCA) utilised as per Policy 6b. Any restrictions should have an accompanying care plan.
Examples of restrictions include: • Ability to leave the ward (should remain on ward for first 24 hours minimum).
• Contact with others
• Movements within ward
• Privacy
• Discharge
• Day to day activities
• Personal care
If an individual lacks the capacity to consent to admission and the admission is completed using the best interest framework then this should be recorded as per policy 6b and an urgent authorisation for a Deprivation of Liberty should be submitted to the Supervisory Body as per the MCA Policy 6b. After 2.5 years held like a restricted prisoner with no respect towards family with one goal and that is to send away – far away from home and family. Best Interest is theirs not my daughter’s and every single capacity assessment is flawed. “Go away my Mum is the NR” “I am not going to engage” – It was their wish to get rid of me as NR only for me to become NR again lol!
Advocacy should be considered and advised to the patients / carers as appropriate upon admission and discharge.
8.3 Consent to Admission for Under 16s’ (Also refer to Chapter 18 (18.3) of the clinical care policy)
Section 131A of the Mental Health Act (1983) requires hospital managers to ensure that patients age 18 or under are admitted to an environment suitable for their age (subject to their need). This duty applies to both detained and informal patients. It is not an absolute prohibition on the admission of such patients. If the young person is deemed competent (Gillick Competency or Fraser Guidelines) and consents to admission it can proceed. Parents and guardians should be kept informed (see chapter 13 of Clinical Care Policy). Total breach of MHA and its Code of Conduct 11:14-11:16.
Where the young person objects to information being shared with a parent or guardian who has parental responsibility then further advice should be sought from the Trust’s safeguarding or legal team. Elizabeth is sharing information such as the assessment that took place for a care home a very long distance away from home.
In cases of a dispute, priority should be given to the ‘parent’ with whom the young person lives or to the court involved. Advice should always be sought from the Trust’s legal team where there is dispute or a lack of clarity. Nothing but court after court and investigation after investigation since I have moved.
Information should be provided to the patient and appropriate family/carers about visiting times, mealtimes, school hours etc. Was told I could only visit evenings but Elizabeth told me other parents were visiting during the day. Now I am completely banned.
8.7 Visitors to LPFT Premises LPFT considers the safety and dignity of all visitors to its premises as extremely important. The link below provides guidance and procedures regarding the management of all visitors to Trust premises and includes process for managing visits by children: Please refer to visitors process within safeguarding policy 11 What they have not done is offer any alternative. If you ban someone from visiting there should be alternative arrangements
In November 2006 the Department of Health launched a ‘Dignity in Care’ campaign with an aim to put dignity and respect at the heart of care services, which extended into Mental health Services in 2007; and is now applicable in all health and social care settings. This campaign, led by the National Dignity Council, identified a 10 point Dignity Challenge to organisations which remains fully applicable today as follows:
1. A zero tolerance to all forms of abuse
2. Supporting people with the same respect you would want for yourself or a member of your family
3. Treat each person as an individual by offering a personalised service
4. Enable people to maintain the maximum possible level of independence, choice and control
5. Listen and support people to express their needs and wants
6. Respect people’s right to privacy
7. Ensure people feel able to complain without fear of retribution
8. Engage with family members and carers as care partners
9. Assist people to maintain confidence and a positive
10. Act to alleviate people’s loneliness and isolation.
9.2 Purpose and scope of this policy 9.2.1 To provide clear information to workers, enabling them to provide care and treatment that respects and maintains patients (service users) rights to privacy and dignity.
9.4 Privacy and Dignity
9.4.1 Privacy refers to freedom from intrusion and relates to all information and practice that is personal or sensitive in nature to an individual.
9.4.2 Dignity refers to how people feel, think and behave in relation to the worth or value of themselves and others. To treat someone with dignity is to treat them as being of worth, in a way that is respectful of them as a valued individual. In care situations, dignity may be promoted or diminished by the physical environment, the organisational culture, by the attitudes and behaviour of the care team and others; and by the way in which activities are carried out. Dignity applies equally to those service users (patients) who have capacity and to those who lack capacity.
9.4.3 Maintaining a service user’s (patient’s) privacy, dignity and respect is central to the delivery of effective health and social care, working in partnership with service users (patients) and where appropriate their carers / families.
9.4.4 Since July 2016 all organisations that provide NHS care or adult social care are legally required to follow the Accessible Information Standard. Meeting the standard requires workers across the Trust to ensure people who have a disability, impairment or sensory loss are provided with information that they can easily read or understand with support, so they can communicate effectively with health and social care services. Sensory issues in Elizabeth’s case who cannot stand crowds, noise and bright lights which makes the current environment totally and utterly unsuitable. She would be better off in a care farm where there are animals, a natural environment but the MDT and commissioners do not see it that way.
9.4.5 The following are examples of how to maintain a service user’s (patient’s) privacy and dignity:
Always ask a service user (patient) which name or title they prefer to be addressed by; and ensure all staff respect the service user’s (patient’s) expressed wishes.
• Ensure the Accessible Information Standard is consistently applied so all patients (service users) and carers where appropriate, are able to effectively access Trust (LPFT) services.
• Ask a patient (service user) if they wish their carer to leave for specific conversations or procedures which may compromise their privacy or dignity.
• Maintain a patient’s privacy when asking or assisting them to dress or undress.
• Close curtains or screens in areas where patients are expected to undress.
• Close observation windows in bedroom doors unless they are being used for observation at that time.
• Obtain informed consent before undertaking examinations or treatments.
• Ensure privacy and confirm the boundaries of confidentiality when discussing any confidential and sensitive issues such as diagnosis, symptomatology, sexual orientation and gender identity.
• Respect privacy and dignity at all times, such as during the delivery of personal care, when undertaking all observational duties, when entering treatment rooms, single sex rooms or bedroom areas, toilets and bathrooms. And do not give prone restraint by several men!
• Always knock or make your entry clear through announcing entry and waiting for a reply before entering* (* except where there is a clinical or care rationale not to do so, which includes during night periods when service users (patients) are sleeping).
• Don’t discuss worker or patient personal information with co-workers whilst carrying out care or within hearing distance of service users (patients), carers and visitors.
• Ensure a service user’s (patient) choice is adhered to in respect of the gender of the staff member carrying out intimate care, such as assisting with washing or undressing.
Ensure reasonable adjustments are made to support a service user (patient) to function at their highest level possible. This may include ensuring a service user (patient) receives timely assessments, such as by a Physiotherapist or Occupational Therapist, and that related prescribed care and / or equipment is provided in a timely manner.
9.9.1 Board of Directors The Board of Directors are responsible for the Trust having policies and procedures in place which meet national and local requirements and / or legislation in order to provide a service which is based on best practice. The lead Director responsible for this policy is the Director of Nursing and Quality Quite frankly what is the point of a Policy when no one takes any notice of it. LPFT would do well to consider OPEN DIALOGUE.
9.9.2 Divisional Managers, Quality Assurance Leads and Team Leaders for in-patient services Divisional Managers, Quality Assurance Leads and Team Leaders for in-patient services are responsible for:
• Monitoring compliance with this policy
• Ensuring timely reporting of any non-compliance of this policy through the DATIX incident reporting system.
• Investigating any reported non-compliance with this policy
• Implementing any actions required following audits, incidents or patient / carer / worker feedback relating to Privacy, dignity and mixed sex accommodation. This may include individual worker development where there is evidence of failure in respect of related practice.
9.9.3 In-patient Ward / Unit Managers and their Deputies In-patient Ward / Unit Managers and their Deputies are responsible for:
• Ensuring workers are aware of this policy, its content, where to access it; and their individual related responsibilities.
• Ensuring timely reporting of any non-compliance of this policy through the DATIX incident reporting system.
• Ensuring timely recording in the service user (patient) record of the date, time and reason for the breach occurring.
• Ensuring service user/s (patient/s) and their carers (where appropriate) receive an apology and an explanation of the reason for the breach.
• Ensuring patient safety is maintained during the period of the breach.
• Ensuring risk assessment/s, care plan/s and observation level/s are closely monitored and reviewed during the period of the breach.
• Ensuring timely escalation within service management structure where support or resource is required to ensure patient safety during the period of the breach.
• Investigating any reported non-compliance with this policy, including taking corrective action to prevent any recurrence.
9.9.4 All workers All workers are responsible for:
• Actively promoting the service user’s (patient’s) privacy and dignity at all times.
• Ensuring that all service users (patients) are cared for with privacy, dignity, and in single sex accommodation (as defined within Section 8.5 of this policy). Page 28 of 642
• Ensuring they are aware of their role to support privacy and dignity including when carrying out practice such as observational work.
• Timely reporting of any breaches of this policy, including those reported to them by service users (patients), carers or other workers through the DATIX incident reporting system.
Associated Documentation
1. NHS 13-14 Standard Contract
2. PL/CNO/2010/3, Professional Letter, Department of Health
3. DSSA Principles, September 2009, Department of Health, Gateway Reference: 12610
4. DSSA in Mental Health and Learning Disabilities, December 2009, Department of Health, Gateway Reference: 12940 5. Assessment of Same Sex Accommodation. Brief Guide for Inspection Teams (CQC 2015). 6. Accessible Information Standard Specification (NHSE 2015).
Staff must be mindful of the impact of mental health conditions on the wider family and support network, not just identified carers and next of kin, ensuring that information is shared as appropriate and wider family members are given the opportunity to seek advice, information and express any concerns they may have. Although it is recognised that the sharing of information may sometimes be difficult, it is crucial to the ongoing wellbeing of both the service users and their carers.
Staff must acknowledge that the carer is frequently the person who knows the service user best, often having regular contact over many years throughout many changes in mental health well-being, social networks and professional support. Not recognised one bit.
The carer is often the person who has to offer support during out-of-hours crises, which can be stressful. By involving the carer in the development of the care plan and crisis plan where appropriate, or ensuring they have a copy of it, the carer can feel supported in assisting the service user to follow it.
Some service users will have entitlement to Section 117 after-care. The elements of the care plan which are provided under this entitlement must be clearly and separately articulated (see Mental Health Act Policy 6a) Help and guidance on assessment and care planning processes can be obtained from the Team Coordinator – Assessment & Care Planning. Application of the Care Programme Approach – CPA Whilst the expression Care Programme Approach was first introduced in mental health services in 1991, since the publication of Refocusing the Care Programme Approach (DoH 2008) the term Care Programme Approach is now specifically used to describe the approach used in secondary mental health care to assess, plan, review and coordinate the range of treatment and support needs for people in contact with secondary mental health services who have complex characteristics as defined below. CPA care and support must be discussed and agreed with the service user and the practitioners involved in the care. Where there is disagreement within the Multi-Disciplinary Team about the level of support from CPA, advice should be sought from relevant clinical leads or managers within the service, such as the Team Leader, Divisional Manager, Quality Lead or Clinical Director. Where there is a disagreement that cannot be resolved, the service user can appeal against the decision
This may be the last blog for some time on my part. What I would like to see is choice and there is none. There is no care in the community and we live in a District where provision is poor although there is a wonderful charitable sector and a lovely community. This would have all benefitted Elizabeth greatly. Like so many other parents and carers I have turned to social media but now I can see I could be doing this for the rest of my life and getting nowhere whatsoever. I am now taking a different route as there is no more choice and also I am one of many affected. It is not right or fair for parents to have to fight fo their sons and daughter’s because of organisational abuse by powerful public bodies.
How Medicine Works and When It Doesn’t: Learning Who to Trust to Get and Stay Healthy Hardcover – 24 Jan. 2023 by F Perry Wilson (Author) 4.5 4.5 out of 5 stars 33 ratings See all formats and editions Blending personal anecdotes with hard science, an accomplished physician, researcher, and science communicator gives you the tools to avoid medical misinformation and take control of your health “A brilliant step toward patients and physicians alike reclaiming a sense of confidence in a system that often feels overwhelming and mismanaged” (Gabby Bernstein, #1 New York Times bestselling author of The Universe Has Your Back).
We live in an age of medical miracles. Never in the history of humankind has so much talent and energy been harnessed to cure disease. So why does it feel like it’s getting harder to live our healthiest lives? Why does it seem like “experts” can’t agree on anything, and why do our interactions with medical professionals feel less personal, less honest, and less impactful than ever?
Through stories from his own practice and historical case studies, Dr. F. Perry Wilson, a physician and researcher from the Yale School of Medicine, explains how and why the doctor-patient relationship has eroded in recent years and illuminates how profit-driven companies–from big Pharma to healthcare corporations–have corrupted what should have been medicine’s golden age. By clarifying the realities of the medical field today, Dr. Wilson gives readers the tools they need to make informed decisions, from evaluating the validity of medical information online to helping caregivers advocate for their loved ones, in the doctor’s office and with the insurance company.
Dr. Wilson wants readers to understand medicine and medical science the way he does: as an imperfect and often frustrating field, but still the best option for getting well. To restore trust between patients, doctors, medicine, and science, we need to be honest, we need to know how to spot misinformation, and we need to avoid letting skepticism ferment into cynicism. For it is only by redefining what “good.
Maria Cristina Patru1 and David H. Reser 2* 1Department of Psychiatry, Hôpitaux Universitaires de Genève, Geneve Switzerland, 2 Department of Physiology, Monash University, Melbourne, Australia Edited by: Bernat Kocsis, Harvard Medical School, USA Reviewed by: Sabina Berretta, McLean Hospital, USA Ami Citri, The Hebrew University, Israel *Correspondence: David Reser david.reser@monash.edu Specialty section: This article was submitted to Schizophrenia, a section of the journal Frontiers in Psychiatry Received: 23 July 2015 Accepted: 26 October 2015 Published: 09 November 2015 Citation: Patru MC and Reser DH (2015) A New Perspective on Delusional States – Evidence for Claustrum Involvement. Front. Psychiatry 6:158. doi: 10.3389/fpsyt.2015.00158
“Delusions are a hallmark positive symptom of schizophrenia, although they are also associated with a wide variety of other psychiatric and neurological disorders.
The heterogeneity of clinical presentation and underlying disease, along with a lack of experimental animal models, make delusions exceptionally difficult to study in isolation, either in schizophrenia or other diseases. To date, no detailed studies have focused specifically on the neural mechanisms of delusion, although some studies have reported characteristic activation of specific brain areas or networks associated with them. Here, we present a novel hypothesis and extant supporting evidence implicating the claustrum, a relatively poorly understood forebrain nucleus, as a potential common center for delusional states.”
Elizabeth’s scan shows a lesion in precisely that area of the brain (marked in blue with red arrow) which needs to be properly identified. See also page three of the PDF paper.
This is directly in the meso-limbic pathway and is associated with delusional behaviour in what some people are still calling schizophrenia.
If you look at page 3 of this paper you will see the brain pictured in coronal, sagittal and horizontal view and the arrows triangulate to where the image/lesion appears in the right hemisphere of her brain on the scan at position 7/24 of the coronal image from the MRI.
This urgently needs looking at by a neurologist and reference needs to be made to this paper.
Whilst commencing to write this blog Elizabeth has just called. She said yesterday that she spent six hours in seclusion whilst being rapidly tranquilised on Xmas Day.
Despite this, Elizabeth did not sound too bad during her supervised phone call. She spoke of escape. By this she clearly said that she escapes in her mind ie dissociation - this is a sign of PTSD for which Elizabeth has never had any treatment for under NHS. Also she has never had underlying pathological tests until I have had to point out the results of the private scan and observations by independent specialists and experts.
With an appointment on the 3 January with a Neurologist that had previously been flatly refused I really do hope that once and for all her whole treatment will be reviewed based upon the findings which clearly indicate the above.
It has been a nightmare to even try to get certain doctors to acknowledge let alone look into something that has been clearly stated in the files going back to 2009. This could all indicate why the treatment has not worked for so many years.
I am very unhappy at the current punishment of having the phone taken away for a trial period. This has already been tried before. I see this as bullying aimed directly at me because I am the one being blamed for the ‘episodes’ that look like fits never seen before even though many of these take place when I am not around. The necessity the MDT believes to be right is completely wrong and has not achieved anything before at Ash Villa except mistrust and upset and nothing is being done in line with the law and correct procedures and now these same restrictions incorporating Xmas is yet again being “tried”.
I hope to put an end to this bullying once and for all as that is how we see it. I am not going to sit back and do nothing whilst this punishment continues for years and years on end as I believe the whole environment of a noisy acute ward to be completely wrong and the whole approach of punishment also.
This is punishment not care. Punishment to stop my daughter from going out to the shop in the hospital grounds, punishment from stopping her listening to her music on her phone by keeping it locked away. What is this achieving? NOTHING but resentment an mistrust and this has been ongoing for one month now with no end in sight.
“Treat people as individuals and uphold their dignity and to do this you must treat people with kindness, respect and compassion and respect and uphold people’s human rights, challenge poor practice and discriminatory attitudes and behaviour relating to their care.
“Act with honesty and integrity at all times, treating people fairly without discrimination, bullying or harassment. Keep to the laws of the country in which you are practising. Never allow someone’s complaint to affect the care that is provided to them.”

)
)


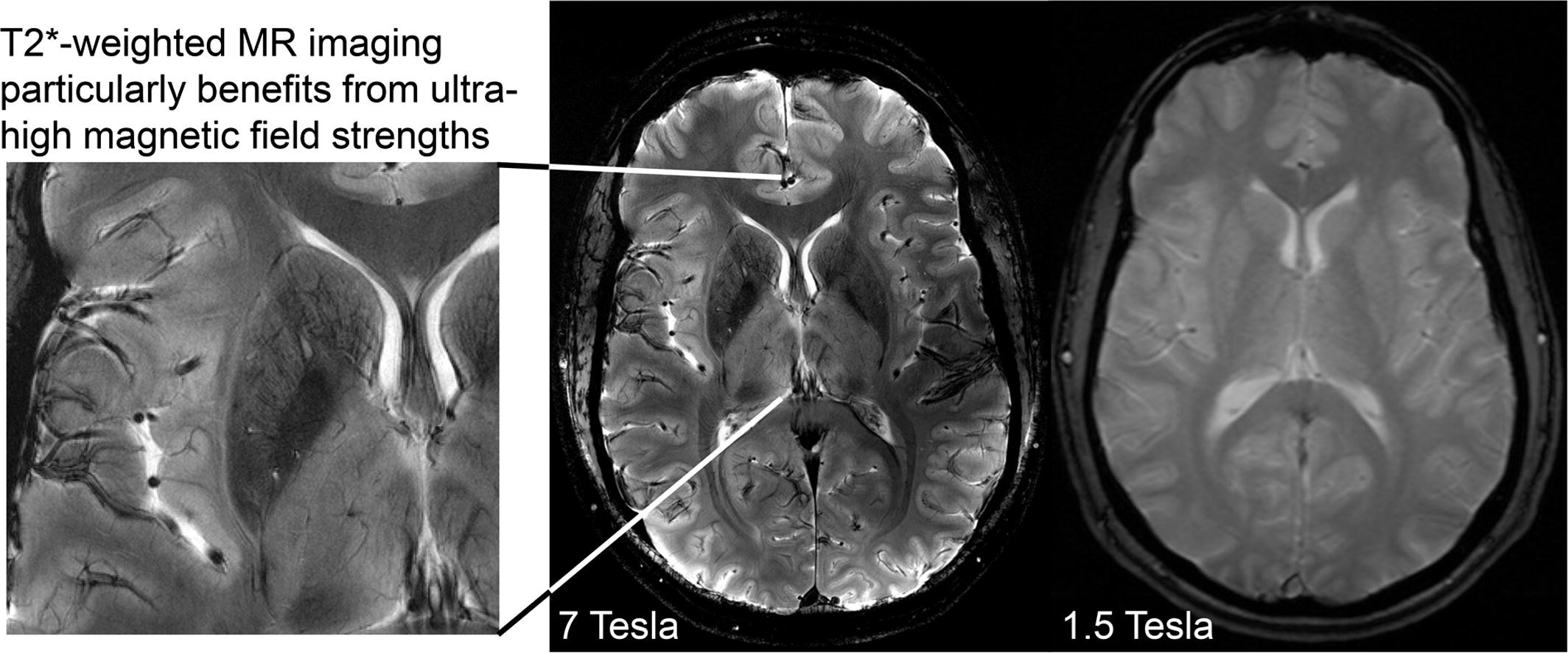

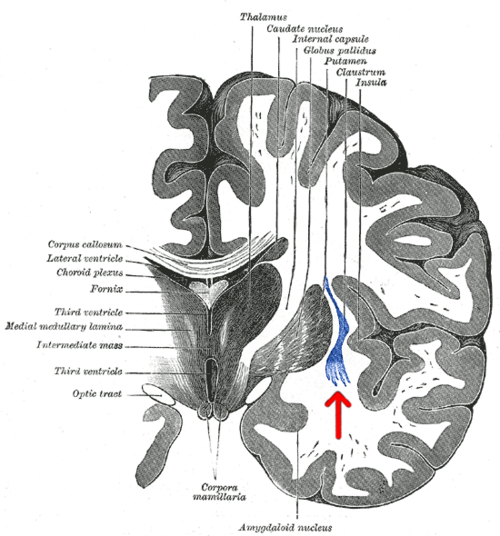

{kind=link}